By Marcello Cherchi, MD PhD
For patients
Head trauma can result in damage to the inner ear, which is sometimes referred to as a “labyrinthine concussion.” This can manifest with hearing loss, tinnitus and disequilibrium. Workup for labyrinthine concussion may include auditory testing, vestibular testing and imaging. There is no specific treatment for labyrinthine concussion. Prognosis is unfavorable, and is worse for hearing than for disequilibrium.
For clinicians
Overview
Labyrinthine concussion refers to labyrinthine damage following head trauma, but without any temporal bone fracture. This damage is usually, though not invariably, ipsilateral to the site of the trauma. The mechanisms of injury may include direct damage from the kinetic energy of a labyrinthine fluid wave, labyrinthine hemorrhage, a traction injury of the vestibulo-cochlear nerve, circulatory disturbances, impaired production/composition of labyrinthine fluid and its flow. The clinician should keep in mind that head trauma can cause not only labyrinthine damage, but also neurological damage. Cases of labyrinthine concussion can present with any combination of auditory and vestibular symptoms. Hearing loss can usually be identified on bedside examination, though should be quantified on audiometry. Ocular motor examination may identify abnormalities, though these have not been well described in the literature; vestibular testing may find a caloric weakness and/or abnormalities in the vestibulo-ocular reflex. Imaging may be normal, though imaging should still be obtained in order to assess for other sequelae of head trauma, such as temporal bone fracture and intracranial hemorrhage. Rare cases of labyrinthine concussion culminate in labyrinthine ossification. There is no specific treatment for labyrinthine concussion. Prognosis for hearing loss is worse than for symptoms of disequilibrium.
Definition
The phrase “labyrinthine concussion” in the literature has come to refer to labyrinthine damage following head trauma, but in the absence of any temporal bone fracture.
The otologic damage from concussion is usually ipsilateral to the site of the trauma, but rare cases describe labyrinthine concussion contralateral to the trauma (Toh, Ho et al. 2010, Villarreal, Mendez et al. 2016), presumably by a contracoup mechanism.
Pathophysiology
The usual mechanisms of disease cited in labyrinthine concussion include direct damage from the kinetic energy of a labyrinthine fluid wave, labyrinthine hemorrhage, or a traction injury of the vestibulocochlear nerve (Bartholomew, Lubner et al. 2020), and there is some evidence in the literature for each process. Less commonly proposed mechanisms include “circulatory disturbances, impaired production and composition of labyrinthine fluid and problems with its outflow” (Chiaramonte, Bonfiglio et al. 2013).
The mechanism of hearing loss in labyrinthine concussion is thought to be, “due to basilar membrane shearing, hair cell degeneration and eventual auditory nerve fiber avulsion” (Chiaramonte, Bonfiglio et al. 2013).
It should also be kept in mind that the actual damage from head trauma need not be restricted to the labyrinth. Since the entire head is concussed, neurological injury should also be considered, and some reports note that in some cases of supposed labyrinthine concussion, the deficits could equally be attributable to “injury to the central auditory pathway (e.g., inferior colliculi or at the upper pontine level)” (Ishai, Knoll et al. 2018).
Presentation
Labyrinthine concussion can manifest with any combination of auditory disturbances (hearing loss, tinnitus) and vestibular symptoms.
Physical examination
The hearing loss in labyrinthine concussion is often detectable on physical examination with usual bedside tests of auditory function, including the finger rub test, Weber test and Rinne test.
Most studies of labyrinthine concussion that report histories of vestibular disturbances do not document an ocular motor examination. One study reported “vertical nystagmus appearing in all positions of the head” (Chiaramonte, Bonfiglio et al. 2013).
Testing: auditory
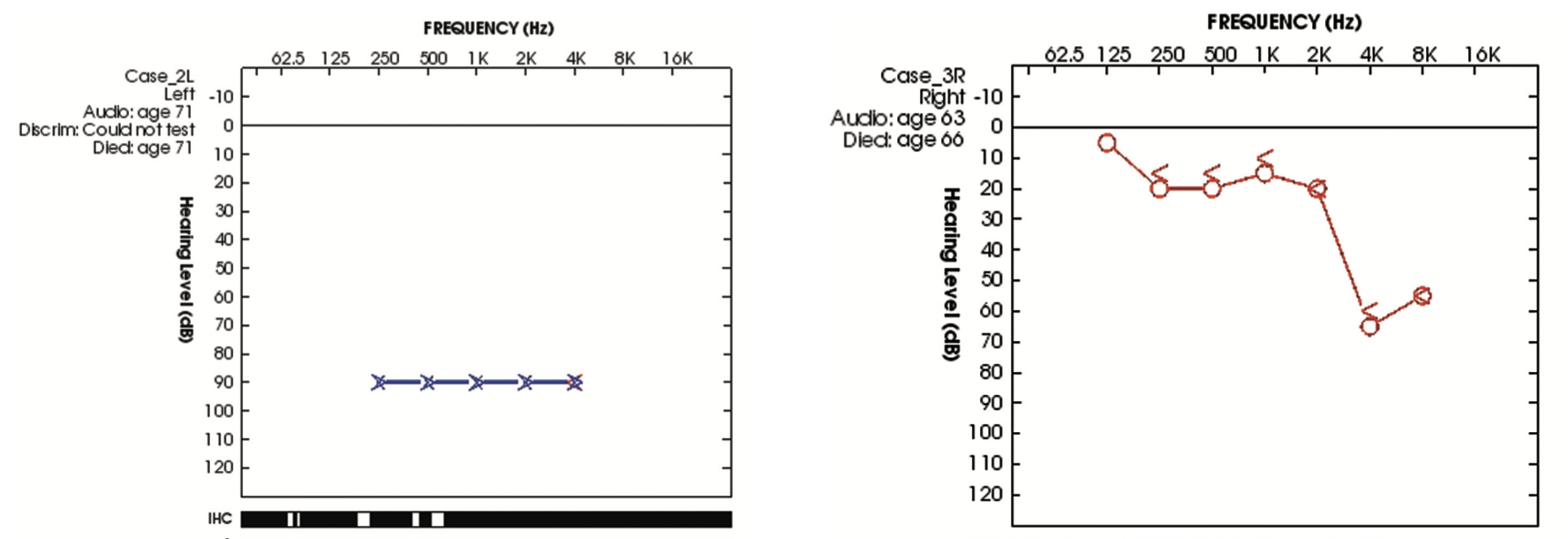
Hearing loss after labyrinthine concussion is variable, ranging “from mild to profound sensorineural hearing loss” (Ishai, Knoll et al. 2018). The hearing loss tends to affect the higher frequencies preferentially (Chiaramonte, Bonfiglio et al. 2013), with some authors noting that, “Labyrinthine concussion in most cases involves a SNHL [sensorineural hearing loss] with a notch in the 4 – 6 kHz resembling acoustic trauma” (Villarreal, Mendez et al. 2016).
The Figure below shows an audiogram from a patient who suffered left-sided labyrinthine concussion in a case reported by Ishai and colleagues (Ishai, Knoll et al. 2018).
Testing: vestibular
Occasional reports include vestibular testing, which “may demonstrate a reduction in the caloric response, vestibulo-ocular reflex gain abnormality and phase after rotational testing” (Chiaramonte, Bonfiglio et al. 2013).
Imaging
Some cases of labyrinthine concussion may have detectable imaging correlates, usually on MRI of the internal auditory canals.
The Figure below, from a case of labyrinthine concussion reported by Chiaramonte and colleagues (Chiaramonte, Bonfiglio et al. 2013), shows right (greater than left) sided T1 hyperintense signal in the cochlea, and right (greater than left) sided contrast enhancement of the cochlea.

Many cases of apparent labyrinthine concussion have no radiographic correlates. However, given that labyrinthine concussion occurs in the context of head trauma, imaging remains an important component of differential diagnosis in order to identify pathologies such as temporal bone fracture and intracranial hemorrhage.
Labyrinthine ossification
Some cases of labyrinthine concussion culminate in labyrinthine ossification (Swartz, Mandell et al. 1985, Schwaber and Tarasidis 1990, Aralasmak, Dincer et al. 2009), though this is relatively rare.
Treatment
Regrettably, “There is no definitive treatment for labyrinthine concussion” (Villarreal, Mendez et al. 2016).
Prognosis
Prognosis of hearing loss after labyrinthine concussion is unfavorable, with most authors concluding that, “ the prognosis of hearing recovery is disappointing in most cases” (Villarreal, Mendez et al. 2016), adding that, “the prognosis for hearing function is worse than for vestibular symptoms” (Chiaramonte, Bonfiglio et al. 2013).
The duration of vestibular symptoms is variable; one paper states that, “The vertigo in these patients can last from several minutes up to several hours” (Chiaramonte, Bonfiglio et al. 2013). However, in cases of labyrinthine concussion that result in labyrinthine ossification, the disequilibrium can last longer; in case described by Aralasmak and colleagues the patient reported “vertigo for the last 20 days” (Aralasmak, Dincer et al. 2009).
Treatment
Insofar as labyrinthine concussion may cause permanent (typically unilateral) auditory and vestibular deficits, patients may benefit from amplification strategies such as a BiCROS (bilateral contralateral routing of signals) hearing aid, or a BAHA (bone attached hearing aid), and from vestibular rehabilitation therapy aimed at unilateral vestibular weakness.
References
Aralasmak A, Dincer E, Arslan G, Cevikol C, Karaali K (2009) Posttraumatic labyrinthitis ossificans with perilymphatic fistulization. Diagn Interv Radiol 15: 239-41. doi: 10.4261/1305-3825.DIR.1621-08.1
Bartholomew RA, Lubner RJ, Knoll RM, Ghanad I, Jung D, Nadol JB, Jr., Alvarez VE, Remenschneider A, Kozin ED (2020) Labyrinthine concussion: Historic otopathologic antecedents of a challenging diagnosis. Laryngoscope Investig Otolaryngol 5: 267-277. doi: 10.1002/lio2.360
Chiaramonte R, Bonfiglio M, D’Amore A, Viglianesi A, Cavallaro T, Chiaramonte I (2013) Traumatic labyrinthine concussion in a patient with sensorineural hearing loss. Neuroradiol J 26: 52-5. doi: 10.1177/197140091302600109
Ishai R, Knoll RM, Chen JX, Wong K, Reinshagen KL, Nadol JB, Jr., Remenschneider AK, Jung DH, Kozin ED (2018) Otopathologic Changes in the Cochlea following Head Injury without Temporal Bone Fracture. Otolaryngol Head Neck Surg 159: 526-534. doi: 10.1177/0194599818769861
Schwaber MK, Tarasidis NG (1990) Labyrinthitis ossificans following post-traumatic hearing loss and vertigo: a case report with antemortem histopathology. Otolaryngol Head Neck Surg 102: 89-91. doi: 10.1177/019459989010200115
Swartz JD, Mandell DM, Faerber EN, Popky GL, Ardito JM, Steinberg SB, Rojer CL (1985) Labyrinthine ossification: etiologies and CT findings. Radiology 157: 395-8. doi: 10.1148/radiology.157.2.3931172
Toh A, Ho EC, Turner N (2010) Contralateral deafness post head injury without temporal bone fractures. Am J Otolaryngol 31: 54-6. doi: 10.1016/j.amjoto.2008.08.010
Villarreal IM, Mendez D, Silva JM, Del Alamo PO (2016) Contralateral Cochlear Labyrinthine Concussion without Temporal Bone Fracture: Unusual Posttraumatic Consequence. Case Rep Otolaryngol 2016: 2123182. doi: 10.1155/2016/2123182
![]()