By Marcello Cherchi, MD PhD
Introduction
After collecting a patient’s data — whether in the form of a specific feature of the clinical history, a particular sign on physical examination, or the result of a specific laboratory test — the degree to which those data influence the suspicion for a given diagnosis may be characterized by sensitivity, specificity, positive and negative predictive values (Monaghan et al. 2021; Parikh et al. 2008). Those statistical characterizations are relevant to clinical practice, but they say nothing about the origin of the certainty/uncertainty of the data or their interpretation.
Any attempt to understand real-world phenomena through scientific analysis must confront uncertainty. The study of this problem is called uncertainty quantification (“UQ”), and intersects with epistemology — the philosophy of knowledge. In the context of healthcare, UQ “is the study of how uncertainties in model inputs affect model outputs” (Tsaneva-Atanasova et al. 2025).
The recognition of uncertainty, and the methods used to address it, greatly influence the biomedical underpinnings of healthcare insofar as they inform our understanding of topics such as (1) how to secure a diagnosis, (2) the mechanistic rationale for a given treatment, and (3) the study of response to treatment. Thus, while UQ is rarely top-of-mind for a practicing clinician, it nevertheless indirectly influences day-to-day clinical decision-making, so it is worth devoting some effort to understanding it.
Uncertainty pervades healthcare at all levels, as schematically illustrated in Figure 1 from Eachempati and colleagues (Eachempati et al. 2022).
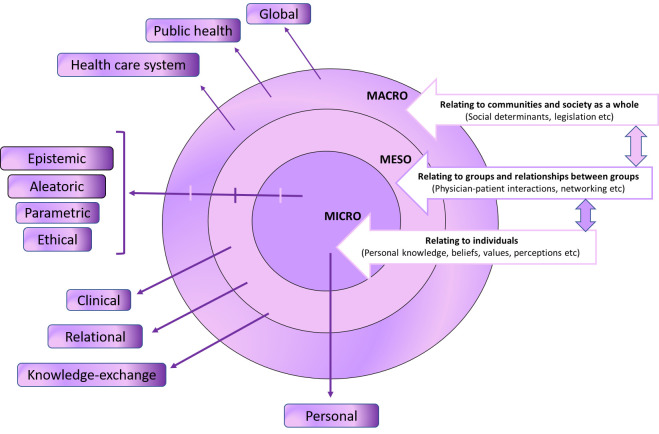
Figure : Interdependent multilevel model of uncertainties in healthcare according to Eachempati and colleagues (Eachempati et al. 2022).
Han (Han et al. 2011) comment that:
“The Merriam-Webster dictionary defines uncertainty as ‘the state of being uncertain,’ and uses a plethora of terms to define ‘uncertain’… Implicit in the dictionary definition of uncertainty as a ‘state’ is a conceptualization of uncertainty as a subjective, cognitive experience of people—a state of mind rather than a feature of the objective world. The defining feature of this state, furthermore, appears to be lack of knowledge about some aspect of reality. Importantly, however, the concept of uncertainty also implies a subjective consciousness or awareness of one’s lack of knowledge, without which one could not feel uncertain; uncertainty is a form of ‘metacognition’—a knowing about knowing” (Han et al. 2011).
Here we will discuss uncertainty as it pertains to diagnosis, while acknowledging the point made by Bhise and colleagues (Bhise et al. 2018) that there is no widely-accepted definition of “diagnostic uncertainty.” Diagnostic uncertainty interfaces with, but is distinct from, the ways in which uncertainty can impact other areas of healthcare, such as uncertainty in medical communication (Han et al. 2019; Kalke et al. 2021), uncertainty in selecting treatment, uncertainty in assessing cost-effectiveness (Bojke et al. 2009), the degree to which uncertainty can be sustained/tolerated (Hillen et al. 2017), and strategies that physicians (Han et al. 2021), trainees (Kim and Lee 2018) and patients (Pienaar and Petersen 2022) use to cope with uncertainty.
There have been many proposed categorizations and taxonomies of uncertainty in medicine (Bhise et al. 2018; Han et al. 2011), though often a proposed classification is developed within the framework of a particular subspecialty. In the following discussion we do not offer a novel framework; rather, we shall simply review several frameworks for thinking about uncertainty, then discuss examples of their application to vestibular physiology and otoneurology.
Framework of first, second and third order uncertainty
One framework for categorizing uncertainty pertains to identifying the “layer” (within a hierarchy) of unknown information that an investigator is trying to confront. This framework classifies uncertainty as first order, second order and third order. This framework is often used in discussions of decision modeling and metrology.
First order uncertainty
First order uncertainty (also called “known unknowns”) is inherent, irreducible randomness or variability in known outcomes even when the probabilities of those outcomes are knowable. First order uncertainty is something “out there in the world,” existing even before any data are collected and interpreted by a model. This type of uncertainty can be statistically quantified (such as by repeated observations), but it is irreducible (cannot be eliminated). The goal in confronting first order uncertainty is to manage known randomness. An everyday example would be the results of a fair coin flip, where the outcomes are known (heads, tails) and the probabilities are known (50% probability of heads, a 50% probability of tails), and there is nothing we can do get any more confident than those probabilistic predictions regarding a single coin flip.
Second order uncertainty
Second order uncertainty (also called “unknown unknowns”) is when the probability distributions themselves are unknown — in other words, there is doubt about the probabilities themselves. This is sometimes described as the possible range of probabilistic distributions — in other words, the distribution of distributions (hence the “second order” nature of this uncertainty). The goal in confronting second order uncertainty is to take into account uncertainty about the model being used. An everyday example would be uncertainty about whether coin is fair or weighted (this is the second-order uncertainty, an “unknown unknown”), which would make it difficult to propose a predictive model with first order uncertainty characteristics (such as whether the probability of landing on each side is 50%, or some other distribution).
Third order uncertainty
Third order uncertainty refers to a more fundamental type of uncertainty resulting from unawareness that one is applying an inappropriate model to analyze a system. This is difficult to address because it is unrecognized. The goal in confronting third order uncertainty is to recognize that the model’s conceptual framework may be entirely mistaken. Reduction of third order uncertainty requires a significant intellectual leap to reframe the problem, which in turn may permit the development of new models for predicting real-world system behavior.
Example of combined first, second and third order uncertainty
A bookstore owner in the 1980s faced different kinds of uncertainty over the decades. Concerns about the activity of competing bookstores would be an example of first order uncertainty. Changes in the broader economy (such as inflation) might be anticipable, and would introduce a second order uncertainty, analysis of which would require taking new variables into account. The emergence of new technology, such as the appearance of the Kindle in 2007, was a dramatic change that would have been unpredictable in the 1980s, and thus its impact on the bookstore owner’s business would represent a third order uncertainty.
Framework based on the investigator’s state (knowledgeable versus ignorant) and the ascertainability of the object of study (knowable versus unknowable)
Some clinical research invokes a framework that relies on an intersection between the dichotomous states of an investigator (who either “knows” or “does not know”) and the dichotomous states of an object of investigation (which is either “knowable” or “unknowable”) (Collins and Cruickshank 2014; Ross Naylor 2010; Shaker and Moore-Clingenpeel 2022; Truesdell et al. 2020). Although Donald Rumsfeld is usually credited with having articulated the permutations of “known knowns,” “known unknowns,” “unknown knowns” and “unknown unknowns” (Rumsfeld 2011), he was apparently drawing on musings already circulating at NASA, and these ideas likely were articulated by earlier thinkers. These permutations, schematically depicted in Table 1, partially overlap with the ontological-aleatoric-epistemic framework that we will discuss below.
Table : Uncertainty framework based on the intersection of “knowing” / “not-knowing” and “knowable” / “not-knowable.”
|
The real-world phenomenon |
|||
|
Is knowable |
Is unknown or unknowable |
||
|
The state of knowledge/ignorance of the investigator |
Investigator knows |
“Known knowns.” The investigator is aware of and understands (knows), a discoverable (knowable) property of the real-world system. This kind of certainty is achievable in completely deterministic systems. |
“Known unknowns.” The investigator is aware (knows) that there is a property of the real-world system that they do not yet fully understand (unknown). This is aleatoric uncertainty. It can be quantified (statistically characterized) but is irreducible (cannot be eliminated). |
|
Investigator does not know (ignorance) |
“Unknown knowns.” The real-world system has discoverable (knowable) properties, but the investigator is currently unaware (ignorant) of them. This is a kind of epistemic ignorance. It can be reduced by collecting additional data. |
“Unknown unknowns.” The investigator is unaware of their own ignorance of a relevant property of the real-world system. This kind of ignorance is poses an ontological problem. Reducing this ignorance requires a significant conceptual shift. |
|
Framework of ontological, aleatoric and epistemic uncertainty
Another framework for categorizing uncertainty pertains to its nature or source. An example of this is the classification of uncertainty as ontological, aleatoric or epistemic. This framework, often referred to as “system-theoretic” (Gansch and Adee 2020), is sometimes used in discussions of risk analysis. These categories partially (but only partially) map on to frameworks mentioned earlier. We will devote more time to discussing this framework because it is more readily applicable to biomedical considerations.
To provide context for this framework, we must say a few words about modeling, and about uncertainty/ignorance.
Modeling
A scientific approach for understanding a real-world system is to develop a model that enables prediction — meaning, a procedure or algorithm that takes a system’s initial state (starting profile of variables), calculates how the system will change, and thereby what the system’s future state (final profile of variables) will be — and then test that model to see how closely its predictions match the real-world system.
A model entails some degree of abstraction from reality, meaning that it must make assumptions and simplifications. Developing a model requires a trade-off between model fit (how well the model’s output matches the data on which it was developed) and model complexity (e.g., how many parameters it takes into account, and how elaborate its calculations are). More complex models require greater computing power. One might think that with unlimited computing power it would be desirable to develop as complex a model as possible (such as by taking into account as many variables as possible), in order to arrive at an extremely close fit with training data; but that approach is not always correct, as it can lead to errors, such as the problem of over-fitting the model to accommodate data outliers (https://dictionary.helmholtz-uq.de/content/modelselection-AICBIC.html), with the result being that when the model is applied to new data, it provides poor predictions. Developing or choosing a model involves finding a balance (in the trade-off between the “model fit” and “model complexity”) that gives acceptable predictive performance at an acceptable computational cost.
An example of the “trade off” between model fit and model complexity comes from ballistics. For everyday purposes, Newtonian mechanics is an adequate model for predicting a projectile’s trajectory, such as the arc of a baseball. We know that this model makes some assumptions, such as treating the entire baseball as if all its mass is concentrated at a single point called the center of gravity. We also know that this model makes some simplifications; for example, it ignores friction with air, it ignores the spin of the baseball, and it ignores the fact that the gravitational force on the baseball changes slightly depending on its altitude. It is possible to develop a model that takes these variables into account, but for most day-to-day purposes, the predictions of that more complex model would not meaningfully differ from the simpler model.
Uncertainty and ignorance
Some philosophical discussions draw a distinction between “uncertainty” and “ignorance,” that will be relevant to this discussion. Birkenholtz and Simon (Birkenholtz and Simon 2022) define ignorance as a “lack of knowledge,” and uncertainty as a “lack of knowledge clarity.” For the purposes of this discussion, we will say that ignorance refers to a circumstance in which the investigator is unaware that they are missing relevant knowledge, whereas uncertainty refers to a circumstance in which the investigator has access to data but is uncertain of how to interpret it (for example, whether it is accurate/precise, whether it is complete, etc.).
An implication of this distinction is that when an investigator is uncertain, then they are aware there is a problem or deficiency that must be rectified, so there is a greater opportunity for improvement. In contrast, when an investigator is ignorant, then they are unaware of potential problems or deficiencies, and thus are not motivated to reconsider their methods and models.
Ontological uncertainty and ignorance
Ontological uncertainty refers to an indeterminacy that is a feature of reality, rather than indeterminacy due to inadequate data (aleatoric uncertainty) or inadequate knowledge (epistemologic ignorance). True ontological uncertainty cannot be reduced by more research or better models. Ontological uncertainty is sometimes regarded as an example of third order uncertainty. Investigators usually cite the Heisenberg uncertainty principle as an example of pure ontological uncertainty — it is a fundamental feature of reality; it is not epistemic since the uncertainty cannot be reduced by augmenting knowledge. Ontological ignorance refers to doubts about the existence of basic categories and entities within a system.
An everyday example of uncertainty resulting from ontological ignorance might be a circumstance in which we thought we were dealing with the output of a coin flip, when in fact the output is coming from a six-sided die (of which we were unaware). Transcending this ontological ignorance requires an investigator coming up with an entirely new idea (a six-sided die).
A basic science example of ontological ignorance would be when the field of physics attempted to model the behavior of subatomic particles using Newtonian mechanics. Transcending this ontological ignorance required theoretical physicists (Neils Bohr, Paul Dirac, Albert Einstein, Werner Heisenberg, Max Planck, Erwin Schrödinger) to come up with an entirely new conceptual framework (quantum mechanics).
A vestibular physiology example of ontological ignorance would be the state of knowledge in the field before Prosper Ménière proposed that vestibular function resided in the ear (Méniere 1861a, b) and Robert Bárány demonstrated the function of the semicircular canals (Bárány 1906, 1907). Transcending this ontological ignorance required these investigators to devise entirely new physiologic concepts.
A final vestibular physiology example of transcending ontological ignorance comes from David Robinson’s pioneering application of control systems analysis in modeling the neurophysiology of eye movements (Robinson 1981).
Aleatoric uncertainty
Aleatoric uncertainty (sometimes also called “stochastic uncertainty” or “data uncertainty”) results from true randomness (noise) in data that is inherent in the phenomenon being studied, or fundamental indeterminacy of the system. This randomness sets the limits of predictability. Eachempati and colleagues comment that:
“Random error is a well-known aspect in scientific research. Although up-to-date evidence informs us on treatment or interventions with a higher probability to show certain effects on the patients, there is a variability in these effects due to random error. The latter can introduce uncertainty in the healthcare context” (Eachempati et al. 2022).
Since the measured real-world phenomena truly vary, aleatoric uncertainty is irreducible by collecting additional data, because those data will still contain the same degree of variability. Aleatoric uncertainty is usually cited as an example of first order uncertainty, in that it involves “known unknowns” — meaning that the investigator is aware (knows) that there is an aspect of the real-world system that can never be completely determined (it remains unknowable).
An everyday example of aleatoric uncertainty — in the sense of stochastic randomness — would be a fair coin flip. The outcomes (heads, tails) are known, and the probabilities (50% for each face) is known, but for a single flip of a fair coin, there is no way to be more certain than this probability; it is irreducible.
A basic science example of aleatoric uncertainty — in the sense of fundamental indeterminacy — would be the quantum mechanical wave-particle duality by which the more confident an observer is about a subatomic particle’s position, the less confident the observer is about that particle’s momentum (and vice versa). This indeterminacy is fundamental and irreducible.
An example from vestibular physiology of aleatoric uncertainty would be the firing of an individual neuron in response to acceleration.
Epistemic uncertainty and ignorance
Epistemic uncertainty (sometimes also called “systemic uncertainty) results from limitations of knowledge. Eachempati and colleagues comment that:
“The source of uncertainty can be limited knowledge or limitations in the quality of knowledge. Moreover, if the knowledge is provided in a way that is not understandable or [is] ambiguous for the receiver or the audience [then] it can lead to uncertainty. Complexity in the information or the context can also lead to uncertainty” (Eachempati et al. 2022).
Epistemic uncertainty can exist at the level of an entire field (“global ignorance”), or at the level of an individual person (“personal ignorance”) (Indrayan 2020). In theory, epistemic uncertainty can be reduced by testing new models, by acquiring more information, or by collecting better data. Epistemic uncertainty is sometimes regarded as an example of second-order uncertainty, in that it involves “unknown unknowns” — meaning that the investigator is unaware of their ignorance about some feature of the real-world system.
A variety of factors can contribute to epistemic uncertainty (Bojke et al. 2009), including data-induced uncertainty, parametric uncertainty, methodological uncertainty, and structural uncertainty (which can include conceptualization and simplification), which lie beyond the scope of this discussion. More information about these is available at https://dictionary.helmholtz-uq.de/content/types_of_uncertainty.html.
An everyday example of epistemic uncertainty would be a coin flip in which we do not know the properties of the coin (such as whether the coin is fair or weighted) and thus we may propose an incorrect model (such as a probabilistic distribution for a fair coin, rather than for a weighted one). This epistemic uncertainty can be reduced by collecting more data (which might reveal a 25% heads — 75% tails probability), which would lead us to refine our model.
A basic science example of epistemic uncertainty would be a case of turbulent flow in fluid dynamics. The real-world system is extremely sensitive to initial conditions, but practically it may not be possible to take all relevant variables into account, so our models will have limited predictive power because of their simplifying assumptions. This epistemic uncertainty can be reduced by collecting more data and/or refining the model (such as by incorporating equations with additional variables).
A vestibular physiology example of epistemic uncertainty would be the “tilt-translation ambiguity,” which arises from the fact that vestibular hair cells are accelerometers, and this neural information alone cannot determine whether sensed acceleration is due to gravity (while the body is at rest) or due to translational movement. The body reduces this epistemic uncertainty by using a more complex model that incorporates other inputs (vision and proprioception).
Another example of reducing epistemic uncertainty in vestibular physiology can be found in the study of the vestibulo-ocular reflex (VOR) from step velocity testing. Modeling this reflex entailed progressive refinements — postulating the direct pathway (mechano-electrical transduction from the semicircular canal ampulla), the indirect pathway (velocity storage mechanism) and adaptation.
A final example, again pertaining to the vestibulo-ocular reflex, comes from the recognition that the accelerometer (and the signal that it generates) is saturable. If one only studied this system within the usual (physiologic) range pf typical head accelerations, then one might conclude that any variability is homoscedastic (i.e., the variability is uniform across all accelerations). But if one were to study responses at higher (supraphysiologic) accelerations, then one would see that the response saturates, and thus the variability is heteroscedastic (non-uniform across all accelerations).
Areas of confusion
It is easy to confuse some cases of aleatoric uncertainty (e.g., outcome of a single coin flip) with ontological uncertainty (e.g., the Heisenberg uncertainty principle). Although both types of uncertainty involve indeterminacy, the distinction pertains to where that uncertainty originates. In aleatoric uncertainty the inherent randomness resides within a known probabilistic model; for example, the behavior of a coin flip can be modeled by classical (Newtonian) physics which in a strict sense is deterministic, but the natural variability in this system’s outcomes results from its extreme sensitivity to initial conditions. In ontological uncertainty the indeterminacy is a fundamental property of the universe itself; for example, the Heisenberg uncertainty principle says that a particle truly does not have a well-defined position and momentum simultaneously; this indeterminacy is not due to a fault in our measurements, but because the particle actually does not exist as a precise point before it is measured, and thus cannot even in principle be fully determined.
It is also easy to confuse some cases of epistemic ignorance with ontological ignorance. The difference stems from whether the “not knowing” arises from a lack of information about a pre-existing reality (epistemic), or from the inherent, fundamental incompleteness of the reality itself (ontological). This is a philosophically interesting difference, but from the perspective of the biomedical investigator trying to solve a problem, these may not be distinguishable.
Summary of the ontological-aleatoric-epistemic framework
A simple schematic of the ontological-aleatoric-epistemic framework is depicted in Figure 2 from Cui and colleagues (Cui et al. 2025).
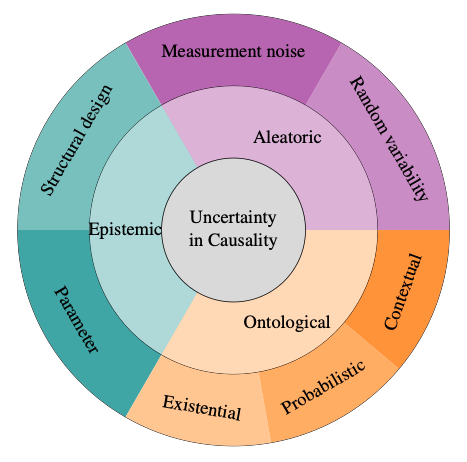
Figure : A concentric view of uncertainty types — aleatoric, epistemic and ontological. Although depicted as conceptually distinct, real-world cases frequently blur these boundaries, highlighting their interwoven nature in practice. From Cui et al (Cui et al. 2025).
The ontological-aleatoric-epistemic- framework for thinking about uncertainty is summarized in Table 2 and Figure 3.
Table : Comparison of aleatoric, epistemic and ontological uncertainty.
|
Type of uncertainty |
Ontological |
Aleatoric |
Epistemic |
|
Similar (but not identical) to |
Third order uncertainty |
First order uncertainty |
Second order uncertainty |
|
Summary |
Ontological uncertainty is “reality-based;” it is a fundamental property of the universe, rather than the result of inadequate measurement (such as from aleatoric uncertainty) or of inadequate understanding (epistemic ignorance). |
Aleatoric uncertainty is “data-based,” arising from true chance in the world. |
Epistemic uncertainty is “knowledge-based,” resulting from ignorance of the real-world system. |
|
Source of uncertainty |
Ontological ignorance (not ontological uncertainty itself) can result from model incompleteness, inappropriate methodology, unrecognized belief systems (e.g., a flawed underlying assumption of the world). |
Inherent randomness (stochasticity) in the real-world system or data-generating process. |
Insufficient data, inadequate modeling, incorrect interpretation. |
|
Reducibility |
Ontological ignorance is difficult to reduce because it currently lies beyond human knowledge or existing models and thus remains unrecognized. Transcending ontological ignorance requires a significant shift in thinking, such as developing a new conceptual framework. |
Can be statistically quantified but not eliminated. It is irreducible by collecting more data or by refining the model because it is an intrinsic property of the real-world system. |
Reducible (at least in theory) by collecting additional data, improving the model, or acquiring more knowledge. |
|
Nature of the uncertainty |
Fundamental doubt about the nature, existence, or categories of things in the real-world system, stemming from different conceptualizations of reality (rather than due merely to inadequate data). |
Objective, natural variance that can often be quantified using probability distributions (e.g., standard deviation). |
A subjective state of knowledge/ignorance due to an agent’s understanding, or due to a model’s internal information state. |
|
Focus of uncertainty |
“What is the thing/model?” Pertains to the entire modeling/analytic framework and its assumptions. |
“What is the random outcome?” Pertains to the frequency of outcomes in repeated trails. |
“What are the true parameters or model?” Pertains to the specific state of the system, or the specific parameter of a model. |
|
Everyday example of uncertainty |
The investigator may believe that a model of a fair die is a valid tool for prediction; but the investigator may be entirely unaware of the possibility that the die is weighted (rigged). |
• The exact outcome of a single flip of a fair coin. • Sensor noise. |
Knowing whether a die is fair or weighted; this is difficult to know from limited data (only a few casts of the die). |
|
Example from basic science |
• Mistakenly applying Newtonian mechanics to try to understand behavior of subatomic particles. This was later replaced by the model of quantum mechanics. • Mistakenly using Hippocrates’ “four humors” mechanism to explain human health and disease. This was later replaced by a model involving anatomy, physiology, chemistry, etc. |
Random decay of a single radioactive atom. We know the statistical probability of decay (half-life) for a large group of radioactive atoms, but we do not know when a specific atom will decay. |
Trying to predict whether the average temperature in a certain region will rise 2˚C or 4˚C. Our models are incomplete; among other problems, we probably do not know all the parameters involved. |
|
Example from vestibular physiology |
• Past: The state of vestibular science before Meniere proposed that the ear mediated vestibular input (Méniere 1861a, b), and before Barany demonstrated the function of semicircular canals (Bárány 1906, 1907). • Future: Perhaps we will discover that humans have significant magnetoreception, and that this is an important parameter in vestibular perception. |
Frequency of firing of an individual vestibular neuron. |
Inability of vestibular otolith organs alone to distinguish between translational acceleration and gravitational acceleration. (Overcoming this epistemic uncertainty requires a model that takes vision and proprioception into account.) |
Figure : Diagram of the ontological-aleatoric-epistemic framework.
Examples of phenomena demonstrating combinations of uncertainty
Real-world phenomena often can be regarded as exhibiting more than one type of uncertainty. Some examples from basic science are shown in Figure 4.
Figure 4: Examples from basic science of phenomena exhibiting more than one type of uncertainty.
Examples of how the different types of uncertainty can influence each other
Each type of uncertainty can influence the others, as shown in Figure 5.
Figure : Examples of how the different types of uncertainty can influence each other.
Examples of the ontological-aleatoric-epistemic framework
We shall review several examples to illustrate the ontological-aleatoric-epistemic framework.
Example: System with one dependent variable and one independent variable
We will illustrate the ontological-aleatoric-epistemic uncertainty framework with a straightforward, tangible example adapted from the technical blog by Andy Jones (https://andrewcharlesjones.github.io/journal/epi-ali-uncertainty.html).
Assume that we have a cartesian plot of data from some real-world phenomenon, as shown in Figure 6, in which 𝑥 is the independent variable, and 𝑦 is the dependent variable.
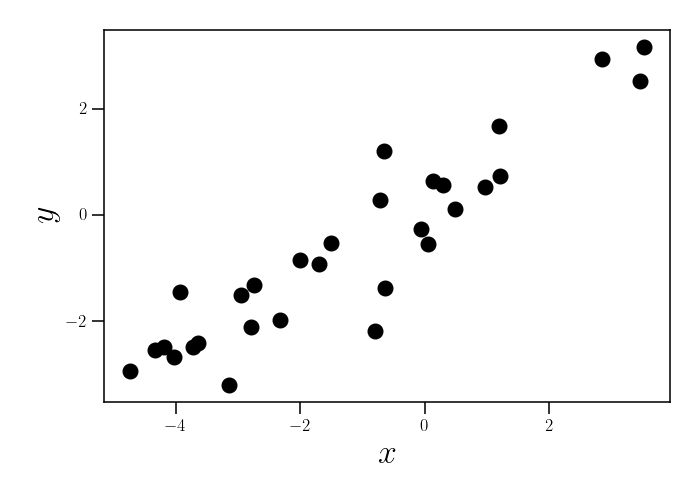
Figure : Scatter plot, in which 𝑥 is the independent variable, and 𝑦 is the dependent variable.
If we assume that the relationship between 𝑥 and 𝑦 is a linear relationship, then we might consider several different linear equations to model that relationship, as shown by the different-colored straight lines in Figure 7.
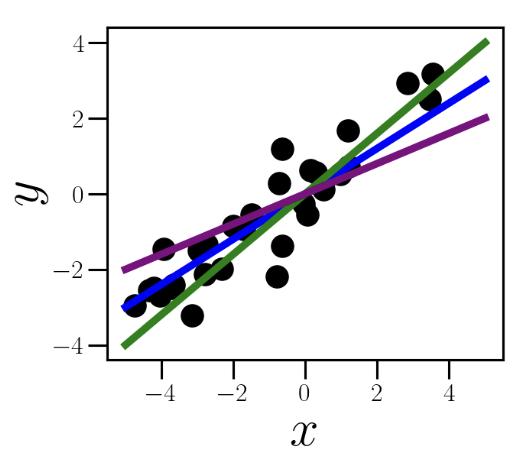
Figure : Scatter plot on which several linear relationships between 𝑥 and 𝑦 has been superimposed.
If we calculate the best-fit line of these data points, then we might arrive at the model in Figure 8. In this model the single blue line is the “best-fit” line which we conclude is most likely to model the relationship between 𝑥 and 𝑦. The real-world variability of the system results in many of the actual data points falling near (but not exactly on) that blue line; these points lie within the broad pink band, which reflects aleatoric (stochastic) uncertainty — the irreducible randomness of the real-world process.
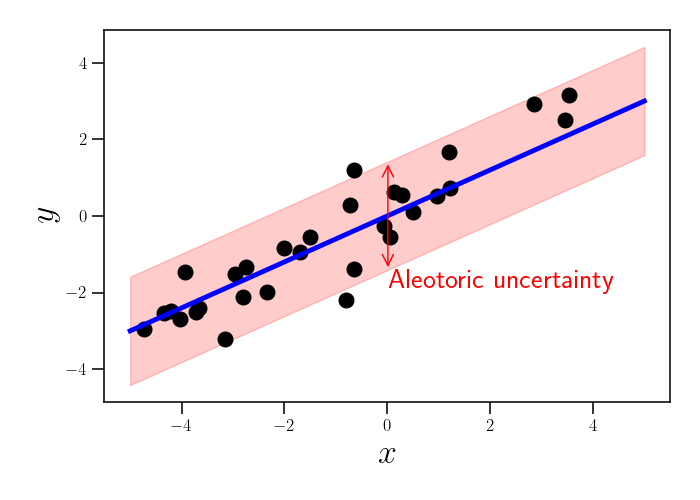
Figure : Scatter plot on which a single best-fit linear relationship is shown. The data fall within the broad pink range. The pink bar reflects aleatoric (stochastic) uncertainty.
But this is a relatively limited set of data. How do we know that the linear equation is the correct model for this real-world relationship? What if we instead used a periodic function, or a cubic function, as shown by the green line and purple line, respectively, in Figure 9?
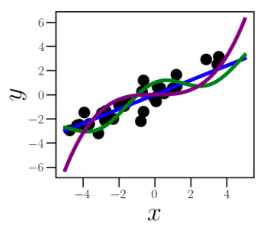
Figure : Scatter plot in which a linear relationship and two non-linear relationships between 𝑥 and 𝑦 have been superimposed. The uncertainty of which model to choose reflects epistemological uncertainty.
This limited set of data does not enable us to make a confident choice of models — specifically, whether this real-world phenomenon should be modeled as a linear function, or as some other function. The fact that we do not know which model to pick reflects epistemic uncertainty. If we collected more data within this range, or if we broadened our search (say to include wider ranges of 𝑥 and 𝑦), or both, then the additional data might reduce the epistemic uncertainty and enable us to choose a model that more accurately reflects observations about the real-world process.
Up to this point in the discussion, we have assumed that we should be using a framework involving a two-dimensional cartesian coordinate system. What if that assumption is mistaken? What if we plotted these data in polar coordinates, and saw a different pattern emerge? Or what if each data point was also associated with one or two additional characteristics (that we had mistakenly considered irrelevant, or that were not available to us), suggesting that we should instead model this system in a three- or four-dimensional space? The fact that we had not even considered these other possible frameworks for modeling the data reflects ontological ignorance.
Examples from vestibular physiology and otoneurology
We review several examples of uncertainty relevant to vestibular physiology and clinical otoneurology
Example: Aleatoric uncertainty in the variability of vestibular hair cell firing
Even if a person moves their head in exactly the same way twice, the firing rate of an individual vestibular neuron may not be identical in each of the two trials, because the firing is not perfectly determined (and thus cannot be perfectly predicted) by the head movement; the neuron’s firing is a probabilistic event influenced by numerous factors (e.g., thermal fluctuations, Brownian motion of endolymph, etc.). This is an example of aleatoric uncertainty at the cellular level.
Example: Reducing epistemic uncertainty through control systems analysis
David Robinson pioneered the application of control systems analysis in modeling the neurophysiology of eye movements (Robinson 1981), offering an entirely novel perspective on its subject, resulting in a field-wide shift in how investigators thought about and studied ocular motor function. In particular, it enabled researchers to propose testable models for eye movements in health and disease. As such, this intellectual shift reflected a significant step in reducing epistemic uncertainty.
Example: Reducing epistemic uncertainty through iterative modeling of the rotational vestibulo-ocular reflex in step velocity testing
Rotatory chair testing (RCT) can test several types of ocular motor function, but it is particularly well suited for studying the rotational vestibulo-ocular reflex (VOR) via protocols known as slow harmonic acceleration (SHA) and step velocity testing (SVT). Our understanding of the rotational VOR evolved as vestibular neurophysiologists iterated through several models to explain the patterns observed in SVT.
Step velocity testing consists of an abrupt, brief, constant acceleration in a given direction, after which the achieved velocity is maintained constant for 30 seconds, then the chair is decelerated in the reverse direction to stop its movement. Most laboratories use an acceleration of 100˚/sec2 for 1 second. Each direction is tested separately.
Figure 10, from Stockwell and Bojrab (Stockwell and Bojrab 1997), diagrams step velocity testing with a leftward stimulus.
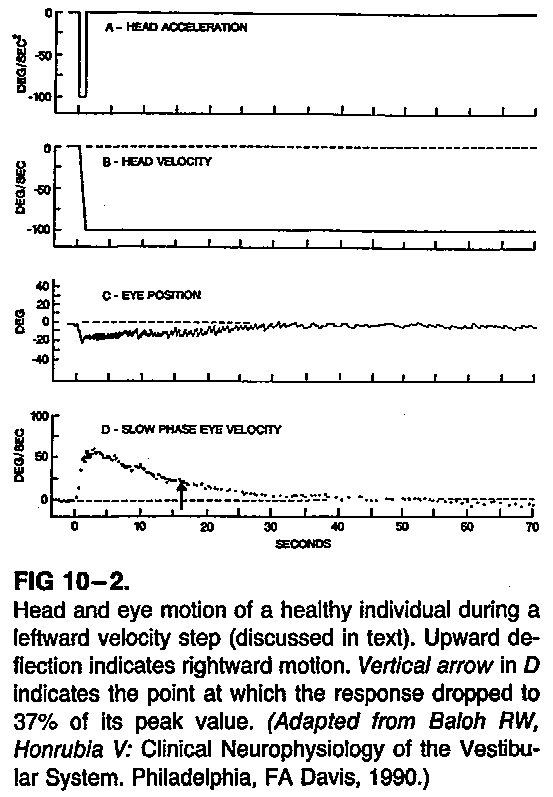
Figure : Normal step velocity testing to the left (Stockwell and Bojrab 1997).
Figure 10 shows abrupt leftward angular acceleration of 100 deg/sec/sec, after which head angular velocity is constant at 100 deg/sec to the left. There is left beat nystagmus, with rightward slow phases. This nystagmus and its slow phase decay over time.
Figure 11, from Guillaud and colleagues (Guillaud et al. 2006), shows the ocular position, velocity and acceleration, tested over several velocities, in step velocity testing.
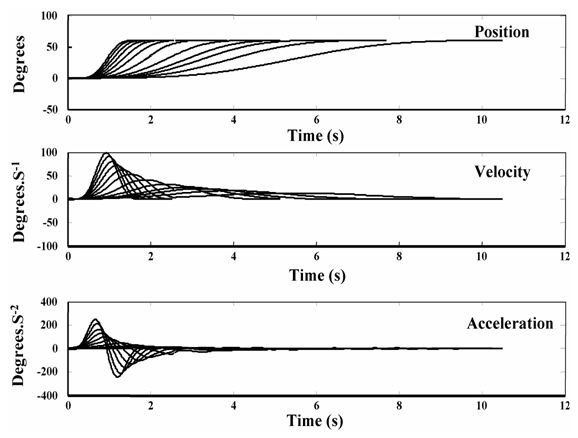
Figure : Results of step velocity testing over a series of velocities (Guillaud et al. 2006).
There are several points to note about Figure 11:
- By about 4 seconds, the traces of eye acceleration are converging.
- This reflects the fact that, as the change in the stimulus (head acceleration) decreases, change in the response (eye acceleration) disproportionately decreases, i.e., becomes more sluggish.
- In other words, the vestibular system is good at detecting large acceleration, and poor at detecting small acceleration.
As Stockwell and Bojrab describe it:
“The system performs well only for relatively fast head motions. The oscillation frequencies used in the slow harmonic acceleration test are at the lower end of its operating range, and therefore, as oscillation frequency decreases, the system becomes less sensitive to the head motion and fails to integrate the head acceleration signal completely, yielding lower gains and greater phase leads” (Stockwell and Bojrab 1997).
The pattern of eye movements induced by step velocity testing is complex. In order to explain it, vestibular physiologists have adapted modeling techniques from engineering. The model comprises three components:
- The mechanical response / direct pathway
- The velocity storage mechanism / indirect pathway
- Adaptation
To understand these components, consider the analogy of a coffee cup. The cup is the bony and membranous labyrinth. The coffee is the endolymph. Picture this sequence of events:
- The coffee cup is rapidly accelerated counterclockwise (looking from above) and then maintains a steady angular velocity in that direction.
- Initially, because of inertia, the coffee remains still (from the perspective of an outside observer).
- Thus, a tiny velocimeter at the edge of the cup (measuring the outermost rim of coffee) would initially measure the angular velocity of the coffee to be equal in amplitude but opposite in direction of the angular velocity of the cup.
- The movement of the coffee lags behind (initially).
- But eventually (because of viscosity) the coffee slowly “catches up” with the motion of the cup. In other words, the coffee reaches the same angular velocity as the cup.
- At this point, the coffee is remaining still relative to the cup. Thus, the tiny velocimeter at the edge of the cup (measuring the outermost rim of coffee) would now measure the angular velocity of the coffee to be zero.
- This is the point at which the angular velocity of the coffee (relative to the cup) has “decayed” to zero.
Everything described so far pertains to the mechanical response of the deflection of the cupula by the endolymph in the lateral semicircular canal. This mechanical response (Stockwell and Bojrab 1997) is sometimes also referred to as the “direct pathway” (Baloh and Honrubia 2001), since its contribution to eye movements is directly proportional to afferents from the cupula. The direct response is mediated by a chain of three neurons, whose cell bodies reside in (1) the vestibular ganglion, (2) the vestibular nuclei, and (3) the oculomotor nuclei.
After the angular acceleration ceases (i.e., the cup is rotating at a constant angular velocity), the endolymph will continue moving for a little while, but shearing forces will soon decelerate it to an angular velocity of zero, and the rate of firing from the cupula will return to baseline — these fluid dynamics and electrophysiology have been experimentally confirmed. It turns out that, even after the angular velocity of the endolymph is zero (and the rate of firing from the cupula has returned to baseline tonic rate), there is still nystagmus for a little while. How can this be?
In order to explain this persistence of nystagmus, vestibular physiologists have postulated a second factor at play, called the velocity storage mechanism (Baloh and Honrubia 2001; Stockwell and Bojrab 1997). This is a positive feedback loop in the central vestibular system that performs the equivalent of mathematical integration of the labyrinthine inputs and yields a response with a time constant (more on this below) longer than that generated by the afferents (from the cupula’s mechanical response). The neural substrate for this is believed to reside in the interneurons mediating the commissural connections between the vestibular nuclei (Katz et al. 1991; Yakushin et al. 2017), though this is controversial. There are other reasons to postulate the existence of this mechanism (such as the normal behavior of optokinetic nystagmus).
The term “velocity storage” is intended to reflect the fact that this mechanism holds, or “stores,” activity from the vestibular periphery and discharges it over a more prolonged time span (i.e., more prolonged than the afferents themselves). For this reason, some refer to it as an “indirect pathway” (Baloh and Honrubia 2001). As discussed above, the vestibular system is generally better at detecting larger accelerations than smaller ones, so from a teleological perspective it is thought that the velocity storage mechanism “improves the ability of the rotational vestibulo-ocular reflexes to transduce the low-frequency components of head rotation” (Leigh and Zee 2015). Since the nystagmus induced by step velocity testing eventually ceases, it is clear that the velocity storage mechanism does not perpetuate the velocity signal forever. Something must cause it to decay.
In order to explain this decay, vestibular physiologists postulated a third factor at play, adaptation. Stockwell and Bojrab (Stockwell and Bojrab 1997) describe adaptation as, “a zero velocity reference level within the central vestibular system that gradually shifts during sustained stimulation in the direction of the ongoing response. Adaptation progressively reduces the strength of a unidirectional response and, after the response finally subsides, induces a response reversal.” The neural substrate of adaptation is unknown.
The three components of step velocity testing are illustrated in the Figure below, from Stockwell and Bojrab (Stockwell and Bojrab 1997).
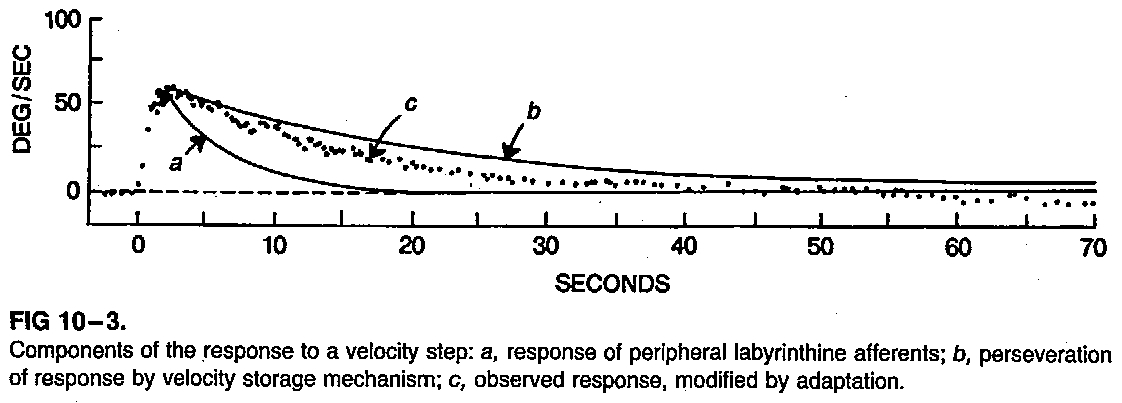
Figure : Components of step velocity testing (Stockwell and Bojrab 1997). In this figure, a = response of peripheral labyrinthine efferents; b = perseveration of response by velocity storage mechanism; c = observed response, modified by adaptation.
In this figure, the output response (plotted dots) is the net result of:
- The mechanical response (direct pathway).
- The velocity storage mechanism (indirect pathway).
- Adaptation.
The example of step velocity testing demonstrates how iterative theoretical corrections (eventually culminating in a result calculated from a composite of the mechanical response, the velocity storage mechanism, and adaptation), diminished epistemic uncertainty, because it resulted in a model that more accurately predicted the behavior of the rotational vestibulo-ocular reflex.
Example: Benign paroxysmal positional vertigo
Mathematical descriptions of what happens in benign paroxysmal positional vertigo (BPPV) can be very elaborate, taking into account properties of the canal (canal radius, duct radius, wall deformability), the endolymph (density, viscosity) and otoliths (shape, size, density) (Obrist and Hegemann 2008), as well as a variety of forces (drag, gravitational force, Coriolis force, centrifugal force, Euler force, vorticeal forces) (Aran-Tapia et al. 2024), and the interactions among the canal, endolymph and otoliths. To make the computational burden more manageable, literature describing otolith behavior and semicircular canal fluid dynamics make a number of simplifying assumptions (Boselli et al. 2013; Joshi et al. 2020; Obrist and Hegemann 2008; Rajguru et al. 2004), such as using idealized anatomical models (e.g., in which a semicircular canal is a perfect torus). Simulators are usually built on such idealized models (Bhandari et al. 2021c).
The biological reality does not conform well to these idealizations in many respects, including even basic geometrical features, such as:
- The semicircular canal lumen is not actually a torus and its cross-sections are not uniform throughout its course (Cortés-Domínguez et al. 2019).
- The canal walls are deformable (Iversen and Rabbitt 2017).
- The semicircular canals are neither truly orthogonal to each other, nor truly planar (Bradshaw et al. 2010).
- The mid-sagittal plane forms an angle of approximately 41˚ with the anterior canal, and an angle of approximately 56˚ with the posterior canal, so the pairs of canals in the so-called RALP (right anterior – left posterior) and LARP (left anterior – right posterior) “planes” are not truly co-planar (Bertholon et al. 2002; Blanks et al. 1975).
- There is anatomical variability from person to person (Della Santina et al. 2005).
- The maximal vestibular response vectors may be distinct from the anatomical canal planes (Ifediba et al. 2007).
These examples of the real-world factors involved in the mechanics and fluid dynamics of benign paroxysmal positional vertigo (BPPV) illustrate that there is still significant epistemic uncertainty in our models of benign paroxysmal positional vertigo (BPPV).
Ontological uncertainty and ignorance
An example of ontological uncertainty in vestibular physiology would be XXX
An example of ontological uncertainty in otoneurology would be whether “dizziness,” “vertigo,” etc. truly constitute a discrete clinical entity. This is an especially pressing question since literature has repeatedly shown that there is no one-to-one correspondence between a particular term and a specific diagnosis (Kerber and Newman-Toker 2015; Newman-Toker and Edlow 2015; Stanton et al. 2007).
Possible examples of ontological ignorance in otoneurology would be whether humans’ limited echolocation abilities (Flanagin et al. 2017; Schornich et al. 2012; Schornich et al. 2013; Thaler and Goodale 2016; Tirado et al. 2021; Wallmeier et al. 2013; Wallmeier et al. 2015) contribute meaningfully to vestibular function (Shayman et al. 2025), or whether humans have magnetoreception abilities (Baker 1988; Shibata et al. 2024; Zhang and Malkemper 2023) that contribute to vestibular processing.
Epistemic uncertainty and ignorance
An example of epistemic uncertainty in vestibular physiology comes from the “tilt-translation ambiguity,” which arises from the fact that otolith vestibular hair cells alone cannot distinguish whether acceleration is the result of gravity (despite the body remaining still) or translational movement. The body reduces this epistemic uncertainty (regarding orientation and motion) by deploying a model that takes other sensory inputs (vision, proprioception) into account.
An example of epistemic uncertainty in otoneurology comes from the day-to-day clinical practice of diagnosing BPPV for cases in which a patient appears to have posterior canal involvement. While isolated posterior canal involvement is a reasonable working diagnosis and appears to be common, it would be difficult to distinguish such a case from one in which there is simultaneous involvement of the posterior and ipsilateral horizontal canals, since posterior canal BPPV often elicits a component of horizontal nystagmus, and that horizontal component would be nearly indistinguishable from the nystagmus elicited by horizontal canal involvement. In fact, cases of so-called “canal conversion” from posterior to horizontal canal BPPV raise the question of whether the initial state was posterior + horizontal canal involvement, and treatment for the posterior canal was successful but the horizontal canal remained active. This scenario reflects two types of uncertainty:
- Aleatoric uncertainty. Our diagnostic tool (infrared video oculography) elicits nystagmus, but we do not have a way to distinguish with confidence whether the pattern reflects posterior canal involvement in isolation, or simultaneous posterior and horizontal canal involvement.
- Epistemic uncertainty. Our diagnostic model assumes that a single canal is involved. This assumption may be mistaken.
What can we do about these uncertainties? Candidate items for a research agenda
Recognizing the different kinds of uncertainty/ignorance is not a purely philosophical exercise; it has practical implications for recognizing what problems remain, which types of uncertainty drive those problems, and how to solve them.
What areas in otoneurology constitute candidate topics for a research agenda or targets for advancing clinical care? Many potential advances leverage technology to reduce aleatoric and epistemic uncertainty, and this probably comprises the “low-hanging fruit.”
A significant data gap in the diagnosis of vestibular disease results from the fact that we do not have good methods for testing the full vestibular tuning spectrum (Cherchi and Yacovino 2021) for all components of the vestibular labyrinth. Current technology enables reasonable assessment of the vestibular tuning spectrum for the horizontal semicircular canals. Future technology, such as magnetic stimulation (Aran-Tapia et al. 2025; Otero-Millan et al. 2017; Roberts et al. 2011; Ward et al. 2017; Ward et al. 2014, 2015; Ward et al. 2019), may make this possible for the vertical canals. This is an example in which we are aware that there is missing knowledge (in the sense of incomplete data) and thus is a case of epistemic uncertainty.
Given the significant anatomical variability between patients of semicircular canal structure mentioned earlier, it may turn out that obtaining a clearer understanding of patient-specific anatomy will enable tailoring maneuvers in a more targeted fashion. This is an area of active research (Rossi-Izquierdo et al. 2025). New imaging technology, such as higher resolution CTs or MRIs, or the use of optical coherence tomography to visualize the labyrinth (Loos et al. 2025), may advance this program. Discerning a patient’s individualized labyrinthine anatomy may improve modeling (reducing epistemic uncertainty) and enable improved data collection (reducing aleatoric uncertainty).
Several areas in clinical otoneurology suffer from a data sampling problem; these tend to arise from diagnoses whose clinical or laboratory manifestations fluctuate, and thus can be difficult to discern from the rare “snapshots” to which the clinician has access during medical encounters. Audiologic examples in this regard are disorders that cause hearing loss that varies, and whose pattern (if discerned) can improve diagnosis, such as the variable sensorineural hearing loss that fluctuates in Meniere’s disease, or is rapid progressive sensorineural hearing loss in autoimmune inner ear disease. Vestibular examples include disorders that cause episodic disequilibrium, such as benign paroxysmal positional vertigo, Meniere’s disease and vestibular paroxysmia. For these auditory and vestibular disorders, otoneurology should learn from other fields, such as endocrinology, in which the advent of continuous glucose monitoring (Vigersky and Shrivastav 2017) has facilitated a paradigm shift in clinical care. Some research in otoneurology is making tentative steps toward home monitoring, such as home audiometry (even if rudimentary, such as with cell phones with ear-bud insert earphones) (Gordon et al. 2005), or home video-oculography (Barreto et al. 2021; Bastani et al. 2025; Bastani et al. 2024; Dobashi et al. 2025; Friedrich et al. 2022; Kiroglu and Dagkiran 2020; Kuroda et al. 2023; Melliti et al. 2023; Parker et al. 2022; Parker et al. 2021; Phillips et al. 2025; Sakazaki et al. 2025; Sookaromdee and Wiwanitkit 2022). Additional opportunities include monitoring of ambulatory function with existing technology (such as step counters, or cell phone gyroscopes (Galan-Mercant and Cuesta-Vargas 2014; Lemoyne et al. 2010; Sun et al. 2014; Umek and Kos 2016)), or developing new technology (such as for-purpose inertial motion sensors (Grouvel et al. 2025; Mohammed et al. 2025)). These are all examples in which we are aware that there is missing knowledge (in the sense of inadequate data sampling), but there are candidate pathways for addressing these gaps — thus they are cases of epistemic uncertainty.
Assessing the utricle may be helpful in the evaluation of unilateral vestibular hypofunction. Approaches to this include measurement of static utricular function (looking for cyclodeviation (Cherchi 2019)) or dynamic utricular function (looking for asymmetries in tilt-induced torsional nystagmus (Sadeghpour et al. 2021)). This would help reduce epistemic uncertainty.
From an instrumentation standpoint, unparalleled spatial and temporal accuracy can be achieved with the dual induction magnetic scleral search coil technique (Collewijn et al. 1975; Reulen and Bakker 1982; Robinson 1963, 1964). However, the expense, and awkwardness of this technology make its use in clinical medicine impractical, thus it is largely restricted to research settings. Research is making progress on refining infrared video oculography, including in the processing of torsional eye movements (Otero-Millan et al. 2015). These advances reduce aleatoric uncertainty.
In studying maneuvers, and in assessing their efficacy, it may be that the accuracy and consistency afforded by mechanical chairs — such as the Epley Omniax (Nakayama and Epley 2005), TRV chair (Richard-Vitton et al. 2005), Rotundum (Bech et al. 2023; Hougaard et al. 2022; Pedersen et al. 2020) or Automated Mechanical Repositioning Treatment chair (Liu et al. 2017; Zhang and Zhu 2023) — will play a useful role. Whether this would have a meaningful effect on treatment outcomes is not yet clear (Chowsilpa et al. 2025). The improved control over conditions (in the form of more precise positioning) may reduce aleatoric uncertainty.
The use of simulators may enhance the study of existing maneuvers (Bhandari et al. 2021a; Bhandari et al. 2021b; Bhandari et al. 2021c; Li et al. 2025; Teixido et al. 2016; Traboulsi and Teixido 2021) and enable the development of new maneuvers (Barreto et al. 2023; Cherchi 2025). Simulators provide improved modeling (reducing epistemic uncertainty).
Ontological ignorance is the most difficult to reduce, as it requires a substantially new way of viewing the system/problem, which usually entails a significant conceptual shift. Previously noted examples include Ménière’s idea that the labyrinth was the locus of vestibular sensation (Méniere 1861a, b); Bárány’s demonstration of semicircular canal function (Bárány 1906, 1907); and David Robinson’s pioneering application of control systems analysis in modeling the neurophysiology of eye movements (Robinson 1981). Such paradigm shifts will come from the imaginations of my successors.
References
Aran-Tapia I, Perez-Munuzuri V, Munuzuri AP, Soto-Varela A, Otero-Millan J, Roberts DC, Ward BK (2025) Modeling of magnetic vestibular stimulation experienced during high-field clinical MRI. Commun Med (Lond) 5: 27. doi: 10.1038/s43856-024-00667-9
Aran-Tapia I, Soto-Varela A, Perez-Munuzuri V, Santos-Perez S, Aran I, Munuzuri AP (2024) Numerical Simulations of the Epley Maneuver With Clinical Implications. Ear Hear 45: 1033-1044. doi: 10.1097/AUD.0000000000001493
Baker RR (1988) Human magnetoreception for navigation. Prog Clin Biol Res 257: 63-80.
Baloh RW, Honrubia V (2001) Clinical Neurophysiology of the Vestibular System, 3rd edn. Oxford University Press, New York
Bárány R (1906) Untersuchungen über den vom Vestibularapparat des Ohres reflektorisch ausgelösten rhythmischen Nystagmus und seine Begleiterscheinungen [Investigations on the rhythmic nystagmus triggered by the vestibular apparatus of the ear and its accompanying symptoms]. Monatschr Ohrenheilk 40: 193-297.
Bárány R (1907) Untersuchungen über das Verhalten des Vestibularapparates bei Kopftraumen und ihre praktische Bedeutng [Studies on the behavior of the vestibular apparatus in head trauma and their practical significance]. Verhandungen der Deutschen otol Gessellschaft: 252-256.
Barreto RG, Yacovino DA, Cherchi M, Nader SN, Teixeira LJ, Silva DAd, Verdecchia DH (2021) The Role of the Smartphone in the Diagnosis of Vestibular Hypofunction: A Clinical Strategy for Teleconsultation during the COVID-19 Pandemic and Beyond. Int Arch Otorhinolaryngol 25: e602-e609. doi: 10.1055/s-0041-1736340
Barreto RG, Yacovino DA, Cherchi M, Teixeira LJ, Nader SN, Leão GF (2023) Universal repositioning maneuver: a new treatment for single canal and multi-canal benign paroxysmal positional vertigo by 3-dimensional model analysis. Journal of International Advanced Otology 19: 242-247. doi: 10.5152/iao.2023.22921
Bastani P, Phillips V, Rieiro H, Otero-Millan J, Zee D, Newman-Toker D, Tehrani A (2025) Feasibility of Using Smartphone Eye-Tracking for Self-recording Positional Tests. Digital Biomarkers: 1-11. doi: 10.1159/000545720
Bastani PB, Rieiro H, Badihian S, Otero‐Millan J, Farrell N, Parker M, Newman‐Toker D, Zhu Y, Saber Tehrani A (2024) Quantifying Induced Nystagmus Using a Smartphone Eye Tracking Application (EyePhone). Journal of the American Heart Association 13: e030927. doi: 10.1161/JAHA.123.030927
Bech MW, Staffe AT, Hougaard DD (2023) A mechanical rotation chair provides superior diagnostics of benign paroxysmal positional vertigo. Front Neurol 14: 1040701. doi: 10.3389/fneur.2023.1040701
Bertholon P, Bronstein AM, Davies RA, Rudge P, Thilo KV (2002) Positional down beating nystagmus in 50 patients: cerebellar disorders and possible anterior semicircular canalithiasis. J Neurol Neurosurg Psychiatry 72: 366-72. doi: 10.1136/jnnp.72.3.366
Bhandari A, Bhandari R, Kingma H, Strupp M (2021a) Diagnostic and Therapeutic Maneuvers for Anterior Canal BPPV Canalithiasis: Three-Dimensional Simulations. Front Neurol 12: 740599. doi: 10.3389/fneur.2021.740599
Bhandari A, Bhandari R, Kingma H, Zuma EMF, Strupp M (2021b) Three-dimensional simulations of six treatment maneuvers for horizontal canal benign paroxysmal positional vertigo canalithiasis. Eur J Neurol 28: 4178-4183. doi: 10.1111/ene.15044
Bhandari A, Kingma H, Bhandari R (2021c) BPPV Simulation: A Powerful Tool to Understand and Optimize the Diagnostics and Treatment of all Possible Variants of BPPV. Front Neurol 12: 632286. doi: 10.3389/fneur.2021.632286
Bhise V, Rajan SS, Sittig DF, Morgan RO, Chaudhary P, Singh H (2018) Defining and Measuring Diagnostic Uncertainty in Medicine: A Systematic Review. J Gen Intern Med 33: 103-115. doi: 10.1007/s11606-017-4164-1
Birkenholtz T, Simon G (2022) Introduction to themed issue: Ignorance and uncertainty in environmental decision-making. Geoforum 132: 154-161. doi: https://doi.org/10.1016/j.geoforum.2021.12.003
Blanks RH, Curthoys IS, Markham CH (1975) Planar relationships of the semicircular canals in man. Acta Otolaryngol 80: 185-96. doi: 10.3109/00016487509121318
Bojke L, Claxton K, Sculpher M, Palmer S (2009) Characterizing structural uncertainty in decision analytic models: a review and application of methods. Value Health 12: 739-49. doi: 10.1111/j.1524-4733.2008.00502.x
Boselli F, Obrist D, Kleiser L (2013) Vortical flow in the utricle and the ampulla: a computational study on the fluid dynamics of the vestibular system. Biomech Model Mechanobiol 12: 335-48. doi: 10.1007/s10237-012-0402-y
Bradshaw AP, Curthoys IS, Todd MJ, Magnussen JS, Taubman DS, Aw ST, Halmagyi GM (2010) A mathematical model of human semicircular canal geometry: a new basis for interpreting vestibular physiology. J Assoc Res Otolaryngol 11: 145-59. doi: 10.1007/s10162-009-0195-6
Cherchi M (2019) Utricular function in vestibular neuritis: a pilot study of concordance/discordance between ocular vestibular evoked myogenic potentials and ocular cycloposition. Exp Brain Res. doi: 10.1007/s00221-019-05529-8
Cherchi M (2025) Unilateral Triple Canal Repositioning Maneuver: Principles and Design. Audiology Research, vol 15. MDPI
Cherchi M, Yacovino DA (2021) Dysfunction along the continuum of vestibulocochlear anatomy, and the corresponding spectrum of clinical presentation: how little we know, and what else we need to learn. Hearing, Balance and Communication: 1-12. doi: 10.1080/21695717.2021.1975984
Chowsilpa S, Chawachat J, Hansudewechakul N, Isaradisaikul SK, Hanprasertpong C (2025) Comparative Effectiveness of the Exact versus Estimated Angle of Head Position in the Epley Maneuver: A Randomized Controlled Trial. Audiol Neurootol 30: 272-281. doi: 10.1159/000543528
Collewijn H, van der Mark F, Jansen TC (1975) Precise recording of human eye movements. Vision Res 15: 447-50. doi: 10.1016/0042-6989(75)90098-x
Collins RA, Cruickshank RH (2014) Known knowns, known unknowns, unknown unknowns and unknown knowns in DNA barcoding: a comment on Dowton et al. Syst Biol 63: 1005-9. doi: 10.1093/sysbio/syu060
Cortés-Domínguez I, Fernández-Seara MA, Perez-Fernandez N, Burguete J (2019) Systematic Method for Morphological Reconstruction of the Semicircular Canals Using a Fully Automatic Skeletonization Process. Applied Sciences 9. doi: 10.3390/app9224904
Cui S, Mouchel L, Faltings B Uncertainty in Causality: A New Frontier Annual Meeting of the Association for Computational Linguistics 2025
Della Santina CC, Potyagaylo V, Migliaccio AA, Minor LB, Carey JP (2005) Orientation of human semicircular canals measured by three-dimensional multiplanar CT reconstruction. J Assoc Res Otolaryngol 6: 191-206. doi: 10.1007/s10162-005-0003-x
Dobashi Y, Noda M, Kuroda T, Miyata N, Ito M, Tsunoda R, Fushiki H (2025) Development of an Eco-Friendly Smartphone-Assisted Nystagmus Recording System for Recording Vertigo Attacks Anytime, Anywhere: Pilot App Development Study. JMIR Form Res 9: e73811. doi: 10.2196/73811
Eachempati P, Buchter RB, Ks KK, Hanks S, Martin J, Nasser M (2022) Developing an integrated multilevel model of uncertainty in health care: a qualitative systematic review and thematic synthesis. BMJ Glob Health 7. doi: 10.1136/bmjgh-2021-008113
Flanagin VL, Schornich S, Schranner M, Hummel N, Wallmeier L, Wahlberg M, Stephan T, Wiegrebe L (2017) Human Exploration of Enclosed Spaces through Echolocation. J Neurosci 37: 1614-1627. doi: 10.1523/JNEUROSCI.1566-12.2016
Friedrich MU, Schneider E, Buerklein M, Taeger J, Hartig J, Volkmann J, Peach R, Zeller D (2022) Smartphone video nystagmography using convolutional neural networks: ConVNG. J Neurol. doi: 10.1007/s00415-022-11493-1
Galan-Mercant A, Cuesta-Vargas AI (2014) Mobile Romberg test assessment (mRomberg). BMC Res Notes 7: 640. doi: 10.1186/1756-0500-7-640
Gansch R, Adee A System Theoretic View on Uncertainties 2020 Design, Automation & Test in Europe Conference & Exhibition (DATE) 2020, pp 1345-1350
Gordon JS, Phillips DS, Helt WJ, Konrad-Martin D, Fausti SA (2005) Evaluation of insert earphones for high-frequency bedside ototoxicity monitoring. J Rehabil Res Dev 42: 353-61. doi: 10.1682/jrrd.2004.06.0093
Grouvel G, Zimmermann T, van de Berg R, Guinand N, Fornos AP, Armand S, Corre J (2025) Assessing dynamic instability in bilateral vestibulopathy patients during daily living tasks using inertial measurement units. Gait & Posture 121: 79-80. doi: https://doi.org/10.1016/j.gaitpost.2025.07.090
Guillaud E, Gauthier G, Vercher JL, Blouin J (2006) Fusion of visuo-ocular and vestibular signals in arm motor control. J Neurophysiol 95: 1134-46. doi: 10.1152/jn.00453.2005
Han PK, Klein WM, Arora NK (2011) Varieties of uncertainty in health care: a conceptual taxonomy. Med Decis Making 31: 828-38. doi: 10.1177/0272989×11393976
Han PKJ, Babrow A, Hillen MA, Gulbrandsen P, Smets EM, Ofstad EH (2019) Uncertainty in health care: Towards a more systematic program of research. Patient Educ Couns 102: 1756-1766. doi: 10.1016/j.pec.2019.06.012
Han PKJ, Strout TD, Gutheil C, Germann C, King B, Ofstad E, Gulbrandsen P, Trowbridge R (2021) How Physicians Manage Medical Uncertainty: A Qualitative Study and Conceptual Taxonomy. Med Decis Making 41: 275-291. doi: 10.1177/0272989X21992340
Hillen MA, Gutheil CM, Strout TD, Smets EMA, Han PKJ (2017) Tolerance of uncertainty: Conceptual analysis, integrative model, and implications for healthcare. Soc Sci Med 180: 62-75. doi: 10.1016/j.socscimed.2017.03.024
Hougaard DD, Valsted SH, Bruun NH, Bech MW, Talebnasab MH (2022) Seven years of experience with treatment of benign paroxysmal positional vertigo with a mechanical rotational chair. Front Neurol 13: 981216. doi: 10.3389/fneur.2022.981216
Ifediba MA, Rajguru SM, Hullar TE, Rabbitt RD (2007) The role of 3-canal biomechanics in angular motion transduction by the human vestibular labyrinth. Ann Biomed Eng 35: 1247-63. doi: 10.1007/s10439-007-9277-y
Indrayan A (2020) Aleatory and epistemic uncertainties can completely derail medical research results. J Postgrad Med 66: 94-98. doi: 10.4103/jpgm.JPGM_585_19
Iversen MM, Rabbitt RD (2017) Wave Mechanics of the Vestibular Semicircular Canals. Biophys J 113: 1133-1149. doi: 10.1016/j.bpj.2017.08.001
Joshi A, Babu D, Prakash AH, Chandrashekara CV (2020) Simulation of endolymph flow for response of cupula. Vibroengineering Procedia 31: 86-90.
Kalke K, Studd H, Scherr CL (2021) The communication of uncertainty in health: A scoping review. Patient Educ Couns 104: 1945-1961. doi: 10.1016/j.pec.2021.01.034
Katz E, Vianney de Jong JM, Buettner-Ennever J, Cohen B (1991) Effects of midline medullary lesions on velocity storage and the vestibulo-ocular reflex. Exp Brain Res 87: 505-20.
Kerber KA, Newman-Toker DE (2015) Misdiagnosing Dizzy Patients: Common Pitfalls in Clinical Practice. Neurol Clin 33: 565-75, viii. doi: 10.1016/j.ncl.2015.04.009
Kim K, Lee YM (2018) Understanding uncertainty in medicine: concepts and implications in medical education. Korean J Med Educ 30: 181-188. doi: 10.3946/kjme.2018.92
Kiroglu M, Dagkiran M (2020) The Role of Mobile Phone Camera Recordings in the Diagnosis of Meniere’s Disease and Pathophysiological Implications. J Int Adv Otol 16: 18-23. doi: 10.5152/iao.2019.6605
Kuroda T, Kuroda K, Fushiki H (2023) Development of a Prototype Video Head Impulse Test System Using an iPhone for Screening of Peripheral Vestibular Dysfunction. Digit Biomark 7: 150-156. doi: 10.1159/000534543
Leigh RJ, Zee DS (2015) The neurology of eye movements, 5th edn. Oxford University Press, Oxford ; New York
Lemoyne R, Mastroianni T, Cozza M, Coroian C, Grundfest W (2010) Implementation of an iPhone as a wireless accelerometer for quantifying gait characteristics. Conf Proc IEEE Eng Med Biol Soc 2010: 3847-51. doi: 10.1109/IEMBS.2010.5627699
Li J, Hu H, Zhang Y, Yang X (2025) Enhancing the security of horizontal canal BPPV repositioning maneuvers: insights from virtual simulation. Front Neurol 16: 1560324. doi: 10.3389/fneur.2025.1560324
Liu X, Treister R, Yan Y, Wang H, Li X (2017) Automated Mechanical Repositioning Treatment for Posterior Canal Benign Paroxysmal Positional Vertigo: A Single-Center Experience and Literature Review. Eur Neurol 78: 240-246. doi: 10.1159/000480429
Loos E, Kerkhofs L, Berg RVd, Desloovere C, Putzeys T, Verhaert N (2025) High-Resolution Visualization of the Human Semicircular Canals Using Optical Coherence Tomography. International Journal of Imaging Systems and Technology 35: e70259. doi: https://doi.org/10.1002/ima.70259
Melliti A, van de Berg M, van de Berg R (2023) Capturing nystagmus during vertigo attacks using a smartphone: adherence, characteristics, pearls and pitfalls. J Neurol. doi: 10.1007/s00415-023-11965-y
Méniere P (1861a) Maladies de l’oreille interne offrant des symptoms de la congestion cerebral apoplectiforme [Diseases of the inner ear presenting with symptoms of apoplectic cerebral congestion]. Gazette Médicale de Paris [Paris Medical Gazette] 16: 88.
Méniere P (1861b) Sur une forme de surdité grave dépendant d’une lésion de l’oreille interne [On a form of severe deafness resulting from damage to the inner ear.]. Bulletin de l’Adadémie Impériale de médecine [Bulletin of the Imperial Academy of Medicine] 26: 241.
Mohammed A, Wang J, Liu X (2025) Wearable Systems for Evaluating Vestibular and Balance Disorders: A Review. IEEE Sensors Journal 25: 37586-37608. doi: 10.1109/JSEN.2025.3605361
Monaghan TF, Rahman SN, Agudelo CW, Wein AJ, Lazar JM, Everaert K, Dmochowski RR (2021) Foundational Statistical Principles in Medical Research: Sensitivity, Specificity, Positive Predictive Value, and Negative Predictive Value. Medicina (Kaunas) 57. doi: 10.3390/medicina57050503
Nakayama M, Epley JM (2005) BPPV and variants: improved treatment results with automated, nystagmus-based repositioning. Otolaryngol Head Neck Surg 133: 107-12. doi: 10.1016/j.otohns.2005.03.027
Newman-Toker DE, Edlow JA (2015) TiTrATE: A Novel, Evidence-Based Approach to Diagnosing Acute Dizziness and Vertigo. Neurol Clin 33: 577-99, viii. doi: 10.1016/j.ncl.2015.04.011
Obrist D, Hegemann S (2008) Fluid-particle dynamics in canalithiasis. J R Soc Interface 5: 1215-29. doi: 10.1098/rsif.2008.0047
Otero-Millan J, Roberts DC, Lasker A, Zee DS, Kheradmand A (2015) Knowing what the brain is seeing in three dimensions: A novel, noninvasive, sensitive, accurate, and low-noise technique for measuring ocular torsion. J Vis 15: 11. doi: 10.1167/15.14.11
Otero-Millan J, Zee DS, Schubert MC, Roberts DC, Ward BK (2017) Three-dimensional eye movement recordings during magnetic vestibular stimulation. J Neurol 264: 7-12. doi: 10.1007/s00415-017-8420-4
Parikh R, Mathai A, Parikh S, Chandra Sekhar G, Thomas R (2008) Understanding and using sensitivity, specificity and predictive values. Indian J Ophthalmol 56: 45-50. doi: 10.4103/0301-4738.37595
Parker TM, Badihian S, Hassoon A, Saber Tehrani AS, Farrell N, Newman-Toker DE, Otero-Millan J (2022) Eye and Head Movement Recordings Using Smartphones for Telemedicine Applications: Measurements of Accuracy and Precision. Front Neurol 13: 789581. doi: 10.3389/fneur.2022.789581
Parker TM, Farrell N, Otero-Millan J, Kheradmand A, McClenney A, Newman-Toker DE (2021) Proof of Concept for an “eyePhone” App to Measure Video Head Impulses. Digit Biomark 5: 1-8. doi: 10.1159/000511287
Pedersen MF, Eriksen HH, Kjaersgaard JB, Abrahamsen ER, Hougaard DD (2020) Treatment of Benign Paroxysmal Positional Vertigo with the TRV Reposition Chair. J Int Adv Otol 16: 176-182. doi: 10.5152/iao.2020.6320
Phillips V, Bastani PB, Rieiro H, Hale DE, Otero-Millan J, Zee DS, Newman-Toker DE, Tehrani AS (2025) A Pilot Study of Smartphone Eye Tracking for Detection of Positional Nystagmus. Digit Biomark 9: 124-129. doi: 10.1159/000547008
Pienaar K, Petersen A (2022) Searching for diagnostic certainty, governing risk: Patients’ ambivalent experiences of medical testing. Sociol Health Illn 44: 25-40. doi: 10.1111/1467-9566.13391
Rajguru SM, Ifediba MA, Rabbitt RD (2004) Three-dimensional biomechanical model of benign paroxysmal positional vertigo. Ann Biomed Eng 32: 831-46. doi: 10.1023/b:abme.0000030259.41143.30
Reulen JP, Bakker L (1982) The measurement of eye movement using double magnetic induction. IEEE Trans Biomed Eng 29: 740-4. doi: 10.1109/TBME.1982.325006
Richard-Vitton T, Seidermann L, Fraget P, Mouillet J, Astier P, Chays A (2005) [Benign positional vertigo, an armchair for diagnosis and for treatment: description and significance]. Rev Laryngol Otol Rhinol (Bord) 126: 249-51.
Roberts DC, Marcelli V, Gillen JS, Carey JP, Della Santina CC, Zee DS (2011) MRI magnetic field stimulates rotational sensors of the brain. Curr Biol 21: 1635-40. doi: 10.1016/j.cub.2011.08.029
Robinson DA (1963) A Method of Measuring Eye Movement Using a Scleral Search Coil in a Magnetic Field. IEEE Trans Biomed Eng 10: 137-45.
Robinson DA (1964) The Measurement of Eye Movement Using Magnetic Induction in a Contact Lens Coil. Biomed Sci Instrum 2: 97-106.
Robinson DA (1981) The use of control systems analysis in the neurophysiology of eye movements. Annu Rev Neurosci 4: 463-503. doi: 10.1146/annurev.ne.04.030181.002335
Ross Naylor A (2010) Known knowns, known unknowns and unknown unknowns: a 2010 update on carotid artery disease. Surgeon 8: 79-86. doi: 10.1016/j.surge.2010.01.006
Rossi-Izquierdo M, Santos-Perez S, Aran-Tapia I, Blanco-Ulla M, Aran-Gonzalez I, Vaamonde-Sanchez-Andrade I, Franco-Gutierrez V, Perez-Munuzuri V, Munuzuri AP, Soto-Varela A (2025) Personalized medicine to treat refractory benign paroxysmal positional vertigo, through computational fluid dynamics analysis from magnetic resonance image reconstructions. Front Neurol 16: 1561356. doi: 10.3389/fneur.2025.1561356
Rumsfeld D (2011) Known and unknown : a memoir. Sentinel, New York
Sadeghpour S, Fornasari F, Otero-Millan J, Carey J, Zee D, Kheradmand A, Motor O, Sadeghpour, Fornasari O-M, Zee K (2021) Evaluation of the Video Ocular Counter-Roll (vOCR) as a New Clinical Test of Otolith Function in Peripheral Vestibulopathy. JAMA Otolaryngology – Head and Neck Surgery. doi: 10.1001/jamaoto.2021.0176
Sakazaki H, Noda M, Dobashi Y, Kuroda T, Tsunoda R, Fushiki H (2025) Monitoring Nystagmus in a Patient With Vertigo Using a Commercial Mini-Infrared Camera and 3D Printer: Cost-Effectiveness Evaluation and Case Report. JMIR Form Res 9: e70015. doi: 10.2196/70015
Schornich S, Nagy A, Wiegrebe L (2012) Discovering your inner bat: echo-acoustic target ranging in humans. J Assoc Res Otolaryngol 13: 673-82. doi: 10.1007/s10162-012-0338-z
Schornich S, Wallmeier L, Gessele N, Nagy A, Schranner M, Kish D, Wiegrebe L (2013) Psychophysics of human echolocation. Adv Exp Med Biol 787: 311-9. doi: 10.1007/978-1-4614-1590-9_35
Shaker M, Moore-Clingenpeel M (2022) The known knowns, known unknowns, and unknown unknowns of surveys and sleep. Ann Allergy Asthma Immunol 129: 669-670. doi: 10.1016/j.anai.2022.09.007
Shayman CS, McCracken MK, Finney HC, Fino PC, Stefanucci JK, Creem-Regehr SH (2025) Integration of auditory and self-motion cues in spatial navigation. J Exp Psychol Hum Percept Perform 51: 664-675. doi: 10.1037/xhp0001316
Shibata T, Hattori N, Nishijo H, Kuroda S, Takakusaki K (2024) The origins of light-independent magnetoreception in humans. Front Hum Neurosci 18: 1482872. doi: 10.3389/fnhum.2024.1482872
Sookaromdee P, Wiwanitkit V (2022) Smartphone, Vestibular Hypofunction, Teleconsultation and COVID-19 Pandemic. Int Arch Otorhinolaryngol 26: e289-e289. doi: 10.1055/s-0042-1744526
Stanton VA, Hsieh YH, Camargo CA, Jr., Edlow JA, Lovett PB, Goldstein JN, Abbuhl S, Lin M, Chanmugam A, Rothman RE, Newman-Toker DE (2007) Overreliance on symptom quality in diagnosing dizziness: results of a multicenter survey of emergency physicians. Mayo Clin Proc 82: 1319-28. doi: 10.4065/82.11.1319
Stockwell CW, Bojrab DI (1997) Background and technique of rotational testing. In: Jacobson GP, Newman CW, Kartush JM (eds) Handbook of Balance Function Testing. Delmar, New York, pp 237-248
Sun B, Wang Y, Banda J (2014) Gait characteristic analysis and identification based on the iPhone’s accelerometer and gyrometer. Sensors (Basel) 14: 17037-54. doi: 10.3390/s140917037
Teixido M, Woods O, Kung B, Seyyedi M (2016) A 3D benign paroxysmal positional vertigo model for study of otolith disease. World J Otorhinolaryngol Head Neck Surg 2: 1-6. doi: 10.1016/j.wjorl.2016.02.002
Thaler L, Goodale MA (2016) Echolocation in humans: an overview. Wiley Interdiscip Rev Cogn Sci 7: 382-393. doi: 10.1002/wcs.1408
Tirado C, Gerdfeldter B, Karnekull SC, Nilsson ME (2021) Comparing Echo-Detection and Echo-Localization in Sighted Individuals. Perception 50: 308-327. doi: 10.1177/03010066211000617
Traboulsi H, Teixido M (2021) BPPV Viewer: A downloadable 3D BPPV model for study of otolith disease. World Journal of Otorhinolaryngology – Head and Neck Surgery 7: 34-39. doi: https://doi.org/10.1016/j.wjorl.2018.10.001
Truesdell AG, Sauer AJ, Alasnag M (2020) Known Knowns, Known Unknowns, and Unknown Unknowns. Cardiovasc Revasc Med 21: 1472-1473. doi: 10.1016/j.carrev.2020.09.023
Tsaneva-Atanasova K, Pederzanil G, Laviola M (2025) Decoding uncertainty for clinical decision-making. Philos Trans A Math Phys Eng Sci 383: 20240207. doi: 10.1098/rsta.2024.0207
Umek A, Kos A (2016) Validation of smartphone gyroscopes for mobile biofeedback applications. Pers Ubiquit Comput 20: 657-666. doi: 10.1007/s00779-016-0946-4
Vigersky R, Shrivastav M (2017) Role of continuous glucose monitoring for type 2 in diabetes management and research. J Diabetes Complications 31: 280-287. doi: 10.1016/j.jdiacomp.2016.10.007
Wallmeier L, Gessele N, Wiegrebe L (2013) Echolocation versus echo suppression in humans. Proc Biol Sci 280: 20131428. doi: 10.1098/rspb.2013.1428
Wallmeier L, Kish D, Wiegrebe L, Flanagin VL (2015) Aural localization of silent objects by active human biosonar: neural representations of virtual echo-acoustic space. Eur J Neurosci 41: 533-45. doi: 10.1111/ejn.12843
Ward BK, Otero-Millan J, Jareonsettasin P, Schubert MC, Roberts DC, Zee DS (2017) Magnetic Vestibular Stimulation (MVS) As a Technique for Understanding the Normal and Diseased Labyrinth. Front Neurol 8: 122. doi: 10.3389/fneur.2017.00122
Ward BK, Roberts DC, Della Santina CC, Carey JP, Zee DS (2014) Magnetic vestibular stimulation in subjects with unilateral labyrinthine disorders. Front Neurol 5: 28. doi: 10.3389/fneur.2014.00028
Ward BK, Roberts DC, Della Santina CC, Carey JP, Zee DS (2015) Vestibular stimulation by magnetic fields. Ann N Y Acad Sci 1343: 69-79. doi: 10.1111/nyas.12702
Ward BK, Roberts DC, Otero-Millan J, Zee DS (2019) A decade of magnetic vestibular stimulation: from serendipity to physics to the clinic. J Neurophysiol 121: 2013-2019. doi: 10.1152/jn.00873.2018
Yakushin SB, Raphan T, Cohen B (2017) Coding of Velocity Storage in the Vestibular Nuclei. Front Neurol 8: 386. doi: 10.3389/fneur.2017.00386
Zhang H, Zhu M (2023) Mechanical rotational chair-assisted multiple canalith repositioning procedures for benign paroxysmal positional vertigo: enhanced vertigo relief, comparable adverse effects, and decreased incidence of residual dizziness. Front Neurol 14: 1226138. doi: 10.3389/fneur.2023.1226138
Zhang L, Malkemper EP (2023) Cryptochromes in mammals: a magnetoreception misconception? Front Physiol 14: 1250798. doi: 10.3389/fphys.2023.1250798
![]()