By Marcello Cherchi, MD PhD
For patients
Dynamic visual acuity testing (DVA) is a bedside examination test that assesses the neurological circuits that connect part of the inner ear’s gyroscope function to certain eye movements. During this test the patient looks at an eye chart and, keeping the head still, reads the farthest line down (with the smallest type) that they can. Then the doctor oscillates the patient’s head with small but quick movements, and while the head is moving, the patient again tries to read the farthest line down that they can — which usually is a line with larger type. If there is a large difference between the line read with the head still and the line read with the head oscillating, then that suggests there may be a problem with a reflex that connects the inner ear gyroscope function to eye movements. This test is not uncomfortable. This test takes about a minute to perform. If you normally wear glasses or contact lenses, then you should also wear them for this test. You do not otherwise need any special preparation for this test.
For clinicians
Overview
The rotational vestibulo-ocular reflex (rVOR) maintains an image stable on the retina despite rotational movements of the head by rotating the eyes an equal amount but in the opposite direction of head movement. The middle frequency range of the vestibular tuning spectrum can be evaluated at the bedside with dynamic visual acuity testing (DVA), sometimes also called the “dynamic illegible ‘E’ test” (Longridge and Mallinson 1984; Sargent et al. 1997). This test is more sensitive for bilateral vestibular weakness than for unilateral vestibular weakness.
Introduction
There are several methods for assessing the rVOR at the bedside, including dynamic visual acuity testing, the ophthalmoscope test, and the head impulse test. Dynamic visual acuity testing and the ophthalmoscope test assess the middle frequency range of the vestibular tuning spectrum, while the head impulse test assesses the high range. Assessment of the low range of the rVOR requires instrumented vestibular testing (such as rotatory chair testing).
Physiology and neuroanatomy
The function of the vestibulo-ocular reflex (VOR) is to stabilize an image on the retina despite rotational and/or translational movements of the head (Rinaudo et al. 2019). Ideally the rotational VOR (rVOR) should rotate the eyes within the orbits by an amount that is equal in magnitude, but opposite in direction, to that of the head, thereby offsetting the head movement and maintaining the point of regard stable on the fovea (in other words, the gain of eye rotation to head rotation is 1.0).
The neuroanatomy of the rVOR is well understood (Bronstein et al. 2015). Dynamic visual acuity testing (to be described in greater detail below) assesses the component of the rotational vestibulo-ocular reflex mediated by the lateral semicircular canals, also called the horizontal rVOR (hrVOR).
Note that the VOR can be assessed for any pair of coplanar semicircular canals; the relevant neuroanatomy is different for each canal (Bronstein et al. 2015).
Equipment needed
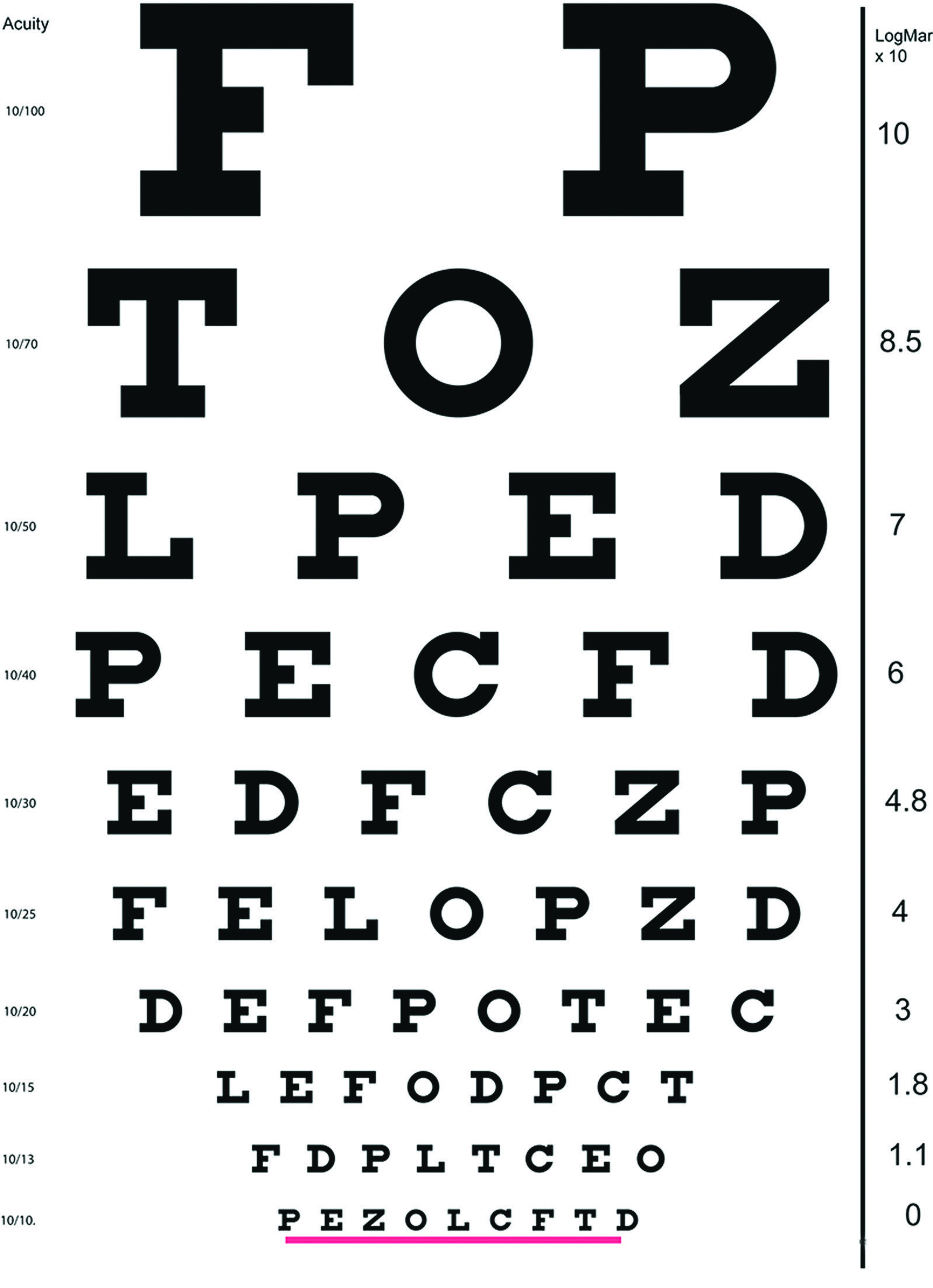
This test requires an eye chart that should be positioned about 12 feet away from the patient (Longridge and Mallinson 1984). Ideally the eye chart should be one calibrated according by LogMAR (logarithm of the minimum angle of resolution), such as that shown in the Figure below, from Hain and Cherchi (Hain and Cherchi 2021).
How to perform the test
If the patient normally wears corrective lenses, then they should do so for this test as well.
First, the patient keeps their head still, looks at the eye chart — placed at a distance of about 12 feet from the patient (Longridge and Mallinson 1984) — and reads the farthest line down that they can.
Second, while the patient is still looking at the eye chart, the examiner passively oscillates the patient’s head (rotating left to right around the vertical axis) at a frequency of about 1.5 Hz (Dannenbaum et al. 2005) to 2 Hz (Eggers and Zee 2003; Huh and Kim 2013). While the patient’s head is in motion, they again read the farthest line down that they can. Reading while the head is oscillating in this fashion cannot rely on visual tracking or smooth pursuit capabilities, which are too slow to process retinal slip at this frequency (Demer et al. 1994; Longridge and Mallinson 1984; Petersen et al. 2013); rather, the eye movements are driven by the vestibulo-ocular reflex, which (when intact) is sufficiently rapid, and can respond to velocities up to 300 deg/sec (Longridge and Mallinson 1984).
Dynamic visual acuity testing is reported as “going from a LogMAR of [A] to [B],” where A is the LogMAR of the farthest line down that the patient can read with the head still, and B is the LogMAR of the farthest line down that the patient can read while the head is oscillating.
What this test assesses
Dynamic visual acuity testing as described above assesses the middle frequency range of the horizontal rVOR, and thus the underlying neuroanatomical pathways of the vestibulo-ocular reflex. A lesion anywhere along this pathway can reduce or abolish the horizontal rVOR, and thus result in poor performance on dynamic visual acuity testing.
How to interpret the test results
A patient with an intact horizontal rVOR may lose up to 2 lines on dynamic visual acuity testing (Kheradmand and Zee 2012; Petersen et al. 2013; Sargent et al. 1997).
If a patient has bilateral vestibular weakness, or significant unilateral vestibular weakness, then they will lose 3 or more lines on dynamic visual acuity testing (Eggers and Zee 2003; Fife et al. 2000; Huh and Kim 2013).
Dynamic visual acuity testing is more sensitive for bilateral vestibular weakness than for unilateral vestibular weakness, though it can detect unilateral vestibular weakness (Dannenbaum et al. 2009) that is sufficiently severe (Longridge and Mallinson 1984).
Limitations
This test requires that the patient have sufficient cervical rotational motion. Patients with cervical vertebral fusions, or significant cervical arthritis or cervicalgia, or other limitations on cervical range of motion, may be unable to perform this test.
Pitfalls
Note that the oscillatory motion in this test is passive (Eggers and Zee 2003); the examiner moves the patient’s head passively because active rotation (i.e., movement under the patient’s volition) slightly improves gain (Della Santina et al. 2002; Goebel et al. 2000), though whether this meaningfully influences test results is unclear (Furmen and Durrant 1998).
If a patient habitually uses corrective refractive lenses (whether spectacles or contact lenses), then they should also wear these during the ophthalmoscope test, otherwise there may be false positive results.
Diseases that may be diagnosed by this test
Dynamic visual acuity testing of the horizontal rotational vestibulo-ocular reflex is particularly helpful in identifying bilateral vestibular weakness, of which there are many etiologies. It is less helpful in identifying unilateral vestibular weakness, which in turn may have many etiologies.
Additional notes
There are computerized versions of dynamic visual acuity testing that may be more accurate (Herdman et al. 1998; Vital et al. 2010), but are not in wide clinical use.
References
Bronstein AM, Patel M, Arshad Q (2015) A brief review of the clinical anatomy of the vestibular-ocular connections-how much do we know? Eye (Lond) 29: 163-70. doi: 10.1038/eye.2014.262
Dannenbaum E, Paquet N, Chilingaryan G, Fung J (2009) Clinical evaluation of dynamic visual acuity in subjects with unilateral vestibular hypofunction. Otol Neurotol 30: 368-72. doi: 10.1097/MAO.0b013e31819bda35
Dannenbaum E, Paquet N, Hakim-Zadeh R, Feldman AG (2005) Optimal parameters for the clinical test of dynamic visual acuity in patients with a unilateral vestibular deficit. J Otolaryngol 34: 13-9. doi: 10.2310/7070.2005.03105
Della Santina CC, Cremer PD, Carey JP, Minor LB (2002) Comparison of head thrust test with head autorotation test reveals that the vestibulo-ocular reflex is enhanced during voluntary head movements. Arch Otolaryngol Head Neck Surg 128: 1044-54.
Demer JL, Honrubia V, Baloh RW (1994) Dynamic visual acuity: a test for oscillopsia and vestibulo-ocular reflex function. Am J Otol 15: 340-7.
Eggers SD, Zee DS (2003) Evaluating the dizzy patient: bedside examination and laboratory assessment of the vestibular system. Semin Neurol 23: 47-58. doi: 10.1055/s-2003-40751
Fife TD, Tusa RJ, Furman JM, Zee DS, Frohman E, Baloh RW, Hain T, Goebel J, Demer J, Eviatar L (2000) Assessment: vestibular testing techniques in adults and children: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 55: 1431-41.
Furmen JM, Durrant JD (1998) Head-only rotational testing in the elderly. J Vestib Res 8: 355-61.
Goebel JA, Isipradit P, Hanson JM (2000) Manual rotational testing of the vestibulo-ocular reflex. Laryngoscope 110: 517-35. doi: 10.1097/00005537-200004000-00004
Hain TC, Cherchi M (2021) Vestibular Testing. CONTINUUM: Lifelong Learning in Neurology 27: 330-347. doi: 10.1212/CON.0000000000000978
Herdman SJ, Tusa RJ, Blatt P, Suzuki A, Venuto PJ, Roberts D (1998) Computerized dynamic visual acuity test in the assessment of vestibular deficits. Am J Otol 19: 790-6.
Huh YE, Kim JS (2013) Bedside evaluation of dizzy patients. J Clin Neurol 9: 203-13. doi: 10.3988/jcn.2013.9.4.203
Kheradmand A, Zee DS (2012) The bedside examination of the vestibulo-ocular reflex (VOR): an update. Rev Neurol (Paris) 168: 710-9. doi: 10.1016/j.neurol.2012.07.011
Longridge NS, Mallinson AI (1984) A discussion of the dynamic illegible “E” test: a new method of screening for aminoglycoside vestibulotoxicity. Otolaryngol Head Neck Surg 92: 671-7.
Petersen JA, Straumann D, Weber KP (2013) Clinical diagnosis of bilateral vestibular loss: three simple bedside tests. Ther Adv Neurol Disord 6: 41-5. doi: 10.1177/1756285612465920
Rinaudo CN, Schubert MC, Figtree WVC, Todd CJ, Migliaccio AA (2019) Human vestibulo-ocular reflex adaptation is frequency selective. J Neurophysiol 122: 984-993. doi: 10.1152/jn.00162.2019
Sargent EW, Goebel JA, Hanson JM, Beck DL (1997) Idiopathic bilateral vestibular loss. Otolaryngol Head Neck Surg 116: 157-62. doi: 10.1016/S0194-59989770318-8
Vital D, Hegemann SC, Straumann D, Bergamin O, Bockisch CJ, Angehrn D, Schmitt KU, Probst R (2010) A new dynamic visual acuity test to assess peripheral vestibular function. Arch Otolaryngol Head Neck Surg 136: 686-91. doi: 10.1001/archoto.2010.99
![]()