By Marcello Cherchi, MD PhD
For patients
Some cases of head trauma cause skull fractures, and some of these skull fractures involve the temporal bone (which contains inner ear structures). Depending on the pattern of the temporal bone fracture, a variety of symptoms can occur, including facial weakness, hearing loss and disequilibrium. Acute care often involves a trauma surgeon, otolaryngologist and neurosurgeon. Almost all patients undergo imaging (such as a temporal bone CT and a brain MRI). Longer-term care may involve an audiologist and vestibular rehabilitation therapy.
For clinicians
Overview
Head trauma may result in skull fractures, and a substantial proportion of these may include temporal bone fractures. Trauma can occur to anyone at any age, but at highest risk are males in their 20s, and these demographics are similar for temporal bone fractures. The most common causes are automobile accidents, assaults and falls. Acute workup includes imaging with high-resolution temporal bone CT and often MRI. There are several classifications of temporal bone fractures, but for otoneurology an important distinction is whether the fracture violates the otic capsule. Immediate presenting features of a temporal bone fracture may include cerebrospinal fluid leaks, facial paralysis, hearing loss, disequilibrium and meningitis. Delayed sequelae include cholesteatoma, meningocele and encephalocele. Acute management often requires involvement of a trauma surgeon, otolaryngologist and neurosurgeon. Audiologic testing can play a role in characterizing hearing loss, and monitoring recovery. If vestibular testing identifies unilateral or bilateral vestibular hypofunction, then vestibular rehabilitation therapy can be considered.
Anatomy
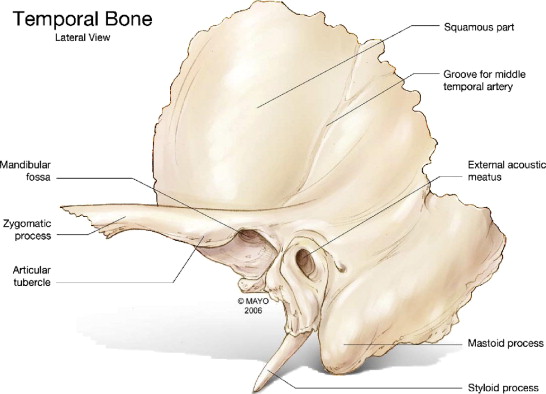
The temporal bone is composed of 5 parts, the squamous, petrous, mastoid, tympanic and styloid portions (Gladwell and Viozzi 2008).
The Figure below, from Gladwell and Viozzi (Gladwell and Viozzi 2008), is an illustration of lateral aspect of the left temporal bone with relevant landmarks.
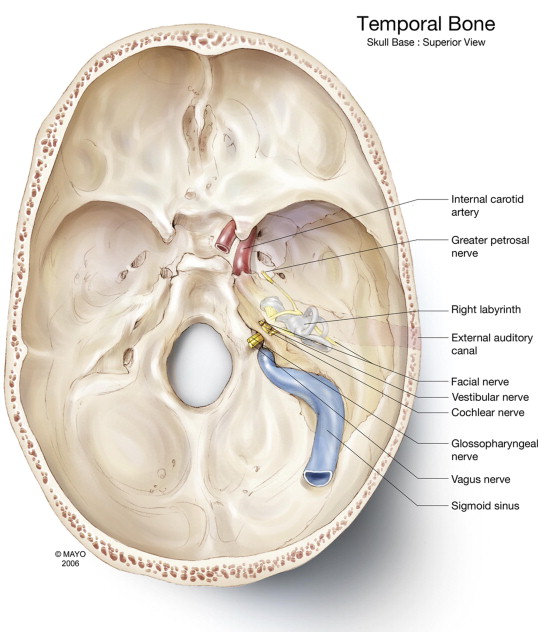
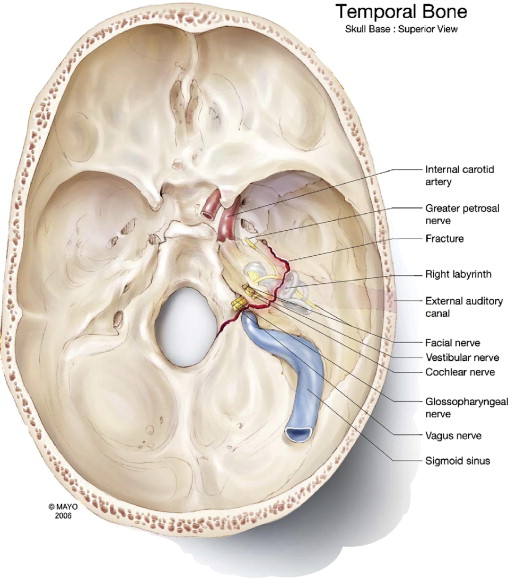
The Figure below, from Gladwell and Viozzi (Gladwell and Viozzi 2008), is an illustration of superior aspect of the skull base, with annotated features of the temporal bone.
Traumatology
Of all patients who have suffered significant head trauma, 23 – 66% involve some type of skull fracture, and 21% have trauma to the skull base (Gladwell and Viozzi 2008).
In patients with any type of skull fracture, from 14 – 22% involve a temporal bone fracture (Brodie and Thompson 1997). Of all cases of temporal bone fracture, bilateral involvement is reported in 9 – 20% of cases (Johnson, Semaan et al. 2008).
The biomechanics of temporal bone fractures have been studied extensively (Yoganandan and Pintar 2004).
Epidemiology
The Chart below from Brodie and Thompson (Brodie and Thompson 1997) reports the etiology of 820 temporal bone fractures in 699 patients.
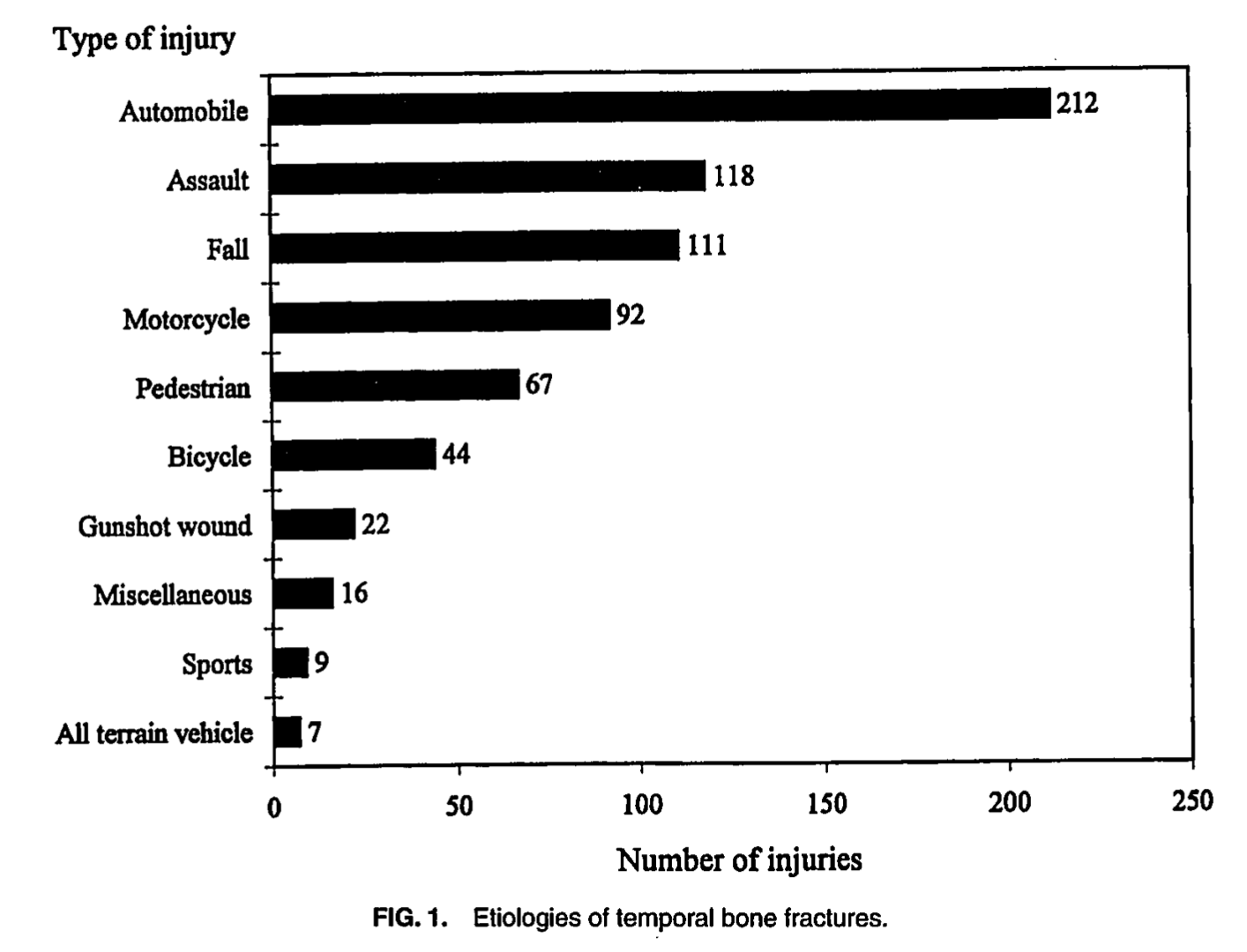
Similar statistics are reported by other investigators (Johnson, Semaan et al. 2008, Saraiya and Aygun 2009).
The Chart below from Brodie and Thompson (Brodie and Thompson 1997), reporting on temporal bone fractures in 699 patients, shows a histogram by age and gender. The peak age at which temporal bone fractures occur is the third decade (age 21 – 30), and is significantly more common in males than in females at all ages.
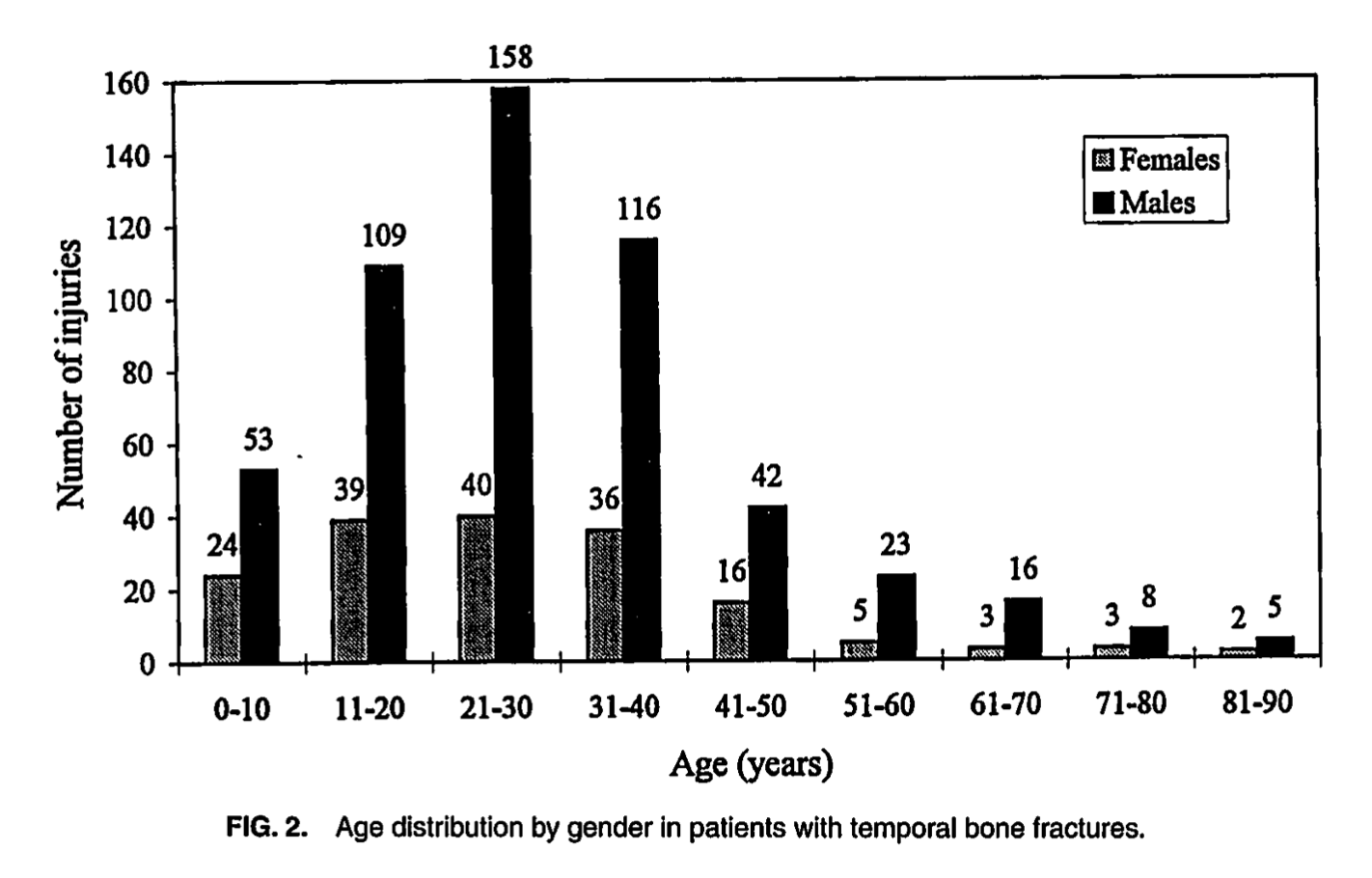
Similar to other types of trauma, “Risk factors for and causes of temporal bone fractures are similar to those in any patient with head injury: younger age, male gender, motor vehicle accidents, falls, recreational injuries, and assaults” (Gladwell and Viozzi 2008).
Presenting features
Temporal bone fractures commonly manifest with cerebrospinal fluid leaks, facial paralysis, sensorineural hearing loss, conductive hearing loss, disequilibrium or meningitis (Brodie and Thompson 1997). Less common sequelae of temporal bone fractures include cholesteatoma and meningocele/encephalocele (Johnson, Semaan et al. 2008). Cholesteatoma may occur at some delay after the original injury, ranging from 2 – 24 years (Ishai, Knoll et al. 2018).
Brodie and Thompson (Brodie and Thompson 1997) report that 2.5% of temporal bone fractures involve the otic capsule, and all such cases cause severe to profound hearing loss.
Brodie and Thompson (Brodie and Thompson 1997) report that of all 699 patients in their series, 24% “complained of some degree of hearing loss.” In 35 patients (5%) the hearing loss was bilateral. Out of 91 patients who had audiometry, 21% had conductive hearing loss, 57% had sensorineural hearing loss, and 22% had mixed hearing loss.
One study reported tinnitus in 41% of patients with temporal bone fractures (Heid, Claussen et al. 2004).
Disequilibrium is reported in 24 – 78% of patients with temporal bone fractures, with mechanisms including otic capsule injury, perilymphatic fistula, labyrinthine concussion, brainstem injury (Gladwell and Viozzi 2008) and traction/shearing injury of the vestibular nerve (Kennedy, Avey et al. 2014, Lantos, Leeman et al. 2019). Other postulated mechanisms include “post-traumatic endolymphatic hydrops” (Johnson, Semaan et al. 2008), for which there is some histopathological evidence (Knoll, Ishai et al. 2020). More mundane causes of disequilibrium following temporal bone fracture include benign paroxysmal positional vertigo (Ishai, Knoll et al. 2018). Several investigators state that “vertigo” following temporal bone fractures is “self-limiting” and resolves “spontaneously” in the range of “6 to 12 months” (Johnson, Semaan et al. 2008, Kennedy, Avey et al. 2014), though these do not cite any data in support of that range, and given the variety of mechanisms, we suspect the range may be broader. One series of 20 patients reported that 10 (50%) complained of vestibular symptoms, and that “the vestibular symptoms improved or disappeared in all cases” (Wennmo and Svensson 1989).
Brodie and Thompson (Brodie and Thompson 1997) report that, of all temporal bone fractures, 7% result in facial paralysis. Of temporal bone fractures involving the otic capsule, 48% also caused facial paralysis; in contrast, fractures that did not involve the otic capsule only resulted in facial paralysis in 6% of cases.
Brodie and Thompson (Brodie and Thompson 1997) report that 122 (17.5%) of 699 patients with temporal bone fracture have a cerebrospinal fluid leak, which included 97 (13.9%) with otorrhea, 16 (2.3%) with rhinorrhea, and 8 (1.1%) with otorrhea.
Brodie and Thompson (Brodie and Thompson 1997) report that of 122 patients who developed a cerebrospinal fluid leak, 9 (7%) developed meningitis. Of the 578 patients without a cerebrospinal fluid fistula, 5 (1%) developed meningitis.
Classification
A variety of classification systems have been proposed for temporal bone fractures (Kennedy, Avey et al. 2014). The most basic one classifies the fractures as either transverse or longitudinal, “based on the relationship of the fracture line to the axis of the petrous ridge and the otic capsule” (Brodie and Thompson 1997). After the orientation of the fracture, the next broad classification pertains to whether or not the fracture involves the otic capsule.
The transverse/longitudinal fracture classification has some utility, but is simplistic. Saraiya and Aygun comment that the, “majority of temporal bone fractures do not fit to this classification system. [The] same anatomic structures may be injured by both types of fractures limiting the clinical value of the classification system in predicting patients’ symptoms and outcome” (Saraiya and Aygun 2009).
Transverse temporal bone fractures usually result from a blow to the occipital region (Swartz 2001), and comprise 10 – 30% of temporal bone fractures (Collins, Krishnamoorthy et al. 2012). Transverse fractures often pass from the foramen magnum across the petrous pyramid and involve the otic capsule, and do not usually affect the ossicular chain or the external auditory canal (Brodie and Thompson 1997).
The Figure below from Gladwell and Viozzi (Gladwell and Viozzi 2008) illustrates a transverse temporal bone fracture involving the otic capsule.
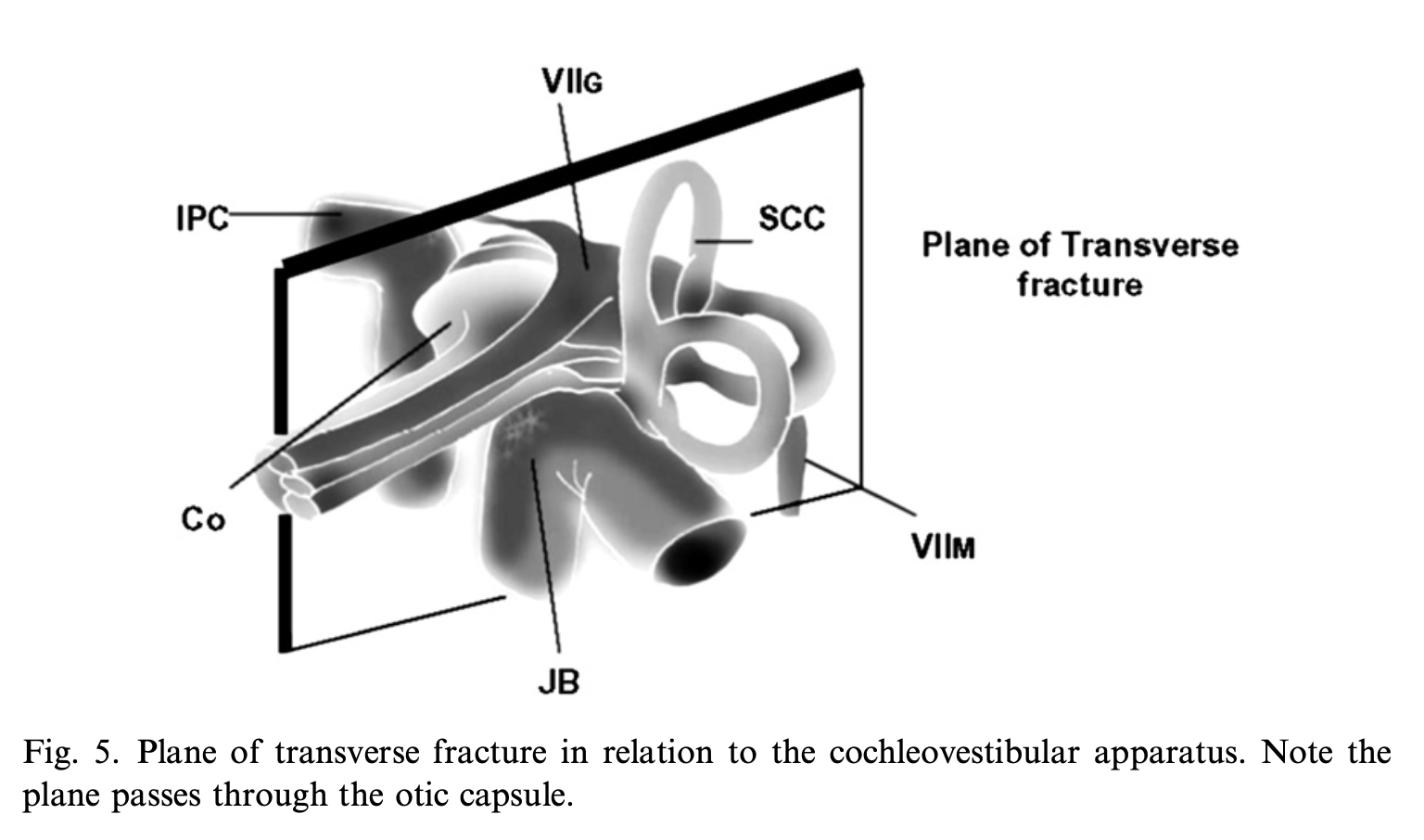
The Figure below from Johnson and colleagues (Johnson, Semaan et al. 2008) is a schematic of a transverse temporal bone fracture passing through the otic capsule.
Longitudinal temporal bone fractures usually result from a blow to temporoparietal region (Swartz 2001), and comprise 70 – 90 % of temporal bone fractures (Collins, Krishnamoorthy et al. 2012). Longitudinal fractures lie anterior to the otic capsule (and thus spare the otic capsule), and involve the squamosal portion of the temporal bone and the posterosuperior wall of the external auditory canal, passing through the mastoid air cells, tegmen mastoideum and tegmen tympani (Brodie and Thompson 1997).
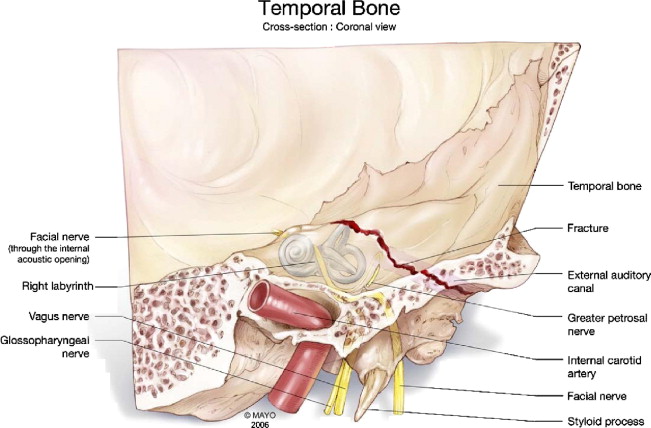
The Figure below from Gladwell and Viozzi (Gladwell and Viozzi 2008) illustrates a longitudinal temporal bone fracture traversing the external auditory canal but sparing the otic capsule.
The Figure below from Johnson and colleagues (Johnson, Semaan et al. 2008) is a schematic of a longitudinal temporal bone fracture passing anterior to the otic capsule.

Diagnostic testing: audiometry
Audiometry is appropriate for any patient with a temporal bone fracture. A longitudinal temporal bone fracture traverses the external auditory canal and can produce conductive hearing loss by several mechanisms (hemotympanum, tympanic membrane perforation, ossicular chain dislocation). A transverse temporal bone fracture can violate the otic capsule and result in severe sensorineural hearing loss (Gladwell and Viozzi 2008).
The incidence of hearing loss reported in temporal bone fractures ranges from 26 – 57% for conductive hearing loss, 14 – 23% for sensorineural hearing loss (including 14% with complete loss), and 20 – 55% for mixed hearing loss. The hearing loss “may be immediate or delayed; may be transient, permanent or progressive” (Johnson, Semaan et al. 2008). Hypothesized mechanisms for progressive hearing loss include perilymphatic fistula and post-traumatic endolymphatic hydrops (Lyos, Marsh et al. 1995).
Given the variability of injury in temporal bone fractures, it is unsurprising that the degree of hearing loss is similarly variable. Suligavi and colleagues (Suligavi, Saiyad et al. 2022) studied a series of patients with temporal bone fractures and found that 34% had mild hearing loss and 3% had severe hearing loss.
In cases of temporal bone fracture that violate the otic capsule and cause sensorineural hearing loss, 1 – 11% of patients eventually develop hearing loss in contralateral (originally un-injured) ear from what is thought to be sympathetic hearing loss (Johnson, Semaan et al. 2008). This is thought to occur because violation of the otic capsule disrupts the blood-labyrinth barrier, exposing labyrinthine antigens to the immune system, which may subsequently mount a maladaptive autoimmune response against the contralateral ear.
Diagnostic testing: vestibular testing
There is little literature specifically on vestibular function in patients who have sustained temporal bone fractures. In our experience, vestibular hypofunction can often be identified (such as with cervical and ocular vestibular evoked myogenic potentials, video head impulse testing, videonystagmography).
Imaging
Patients presenting to an emergency room with trauma will generally undergo a noncontrast head CT. In order to identify and characterize a temporal bone fracture, a high-resolution temporal bone CT (with <1 mm collimation) with multiplanar reconstructions is more helpful (Kurihara, Fujikawa et al. 2020). High-resolution CT is particularly helpful for smaller structures, and is well-suited for identifying ossicular fractures and ossicular chain dislocations.
In the context of trauma, an MRI of the brain (and probably also cervical spine) is usually desirable to evaluate nervous system structures and other soft tissues. MRI is also helpful for distinguishing fluid from air, and identifying hemorrhage (Kurihara, Fujikawa et al. 2020).
When reviewing radiology studies of the temporal bone in a patient who has suffered head trauma it is important to keep in mind that many normal features may mimic fractures (Kwong, Yu et al. 2012). Broadly, “many normal structures are linear and may mimic fracture lines. These mimics include aqueducts, canaliculi, grooves, suture, fissures and other entities” (Kurihara, Fujikawa et al. 2020).
Histopathology
Individual case reports describe various degenerative changes in the vestibular system (Benitez, Bouchard et al. 1980). Temporal bone series from patients who suffered temporal bone fractures involving the otic capsule describe distinct degenerative changes in vestibular hair cells, Scarpa’s ganglion, and the vestibular nerve (Knoll, Ishai et al. 2020).
Treatment
Management of temporal bone fractures almost always requires a multi-disciplinary approach. Acute management often involves a trauma surgeon, otolaryngologist, neurosurgeon, and intensivist (or neuro-intensivist). Longer-term management may involve otolaryngology, neurology, audiology and physical therapy. Depending on what other injuries occurred, other disciplines may be necessary.
As far as otoneurology and vestibular medicine are concerned, auditory deficits are usually monitored and managed by audiology. Vestibular deficits are usually managed with vestibular physical therapy, though the specific strategies will depend on the lesion(s) involved (for example, benign paroxysmal positional vertigo, vestibular hypofunction).
References
Benitez JT, Bouchard KR, Lane-Szopo D (1980) Pathology of deafness and disequilibrium in head injury:a human temporal bone study. Am J Otol 1: 163-7.
Brodie HA, Thompson TC (1997) Management of complications from 820 temporal bone fractures. Am J Otol 18: 188-97.
Collins JM, Krishnamoorthy AK, Kubal WS, Johnson MH, Poon CS (2012) Multidetector CT of temporal bone fractures. Semin Ultrasound CT MR 33: 418-31. doi: 10.1053/j.sult.2012.06.006
Gladwell M, Viozzi C (2008) Temporal bone fractures: a review for the oral and maxillofacial surgeon. J Oral Maxillofac Surg 66: 513-22. doi: 10.1016/j.joms.2007.08.039
Heid L, Claussen CF, Kersebaum M, Nagy E, Bencze G, Bencsik B (2004) Vertigo, dizziness, and tinnitus after otobasal fractures. Int Tinnitus J 10: 94-100.
Ishai R, Knoll RM, Chen JX, Wong K, Reinshagen KL, Nadol JB, Jr., Remenschneider AK, Jung DH, Kozin ED (2018) Otopathologic Changes in the Cochlea following Head Injury without Temporal Bone Fracture. Otolaryngol Head Neck Surg 159: 526-534. doi: 10.1177/0194599818769861
Johnson F, Semaan MT, Megerian CA (2008) Temporal bone fracture: evaluation and management in the modern era. Otolaryngol Clin North Am 41: 597-618, x. doi: 10.1016/j.otc.2008.01.006
Kennedy TA, Avey GD, Gentry LR (2014) Imaging of temporal bone trauma. Neuroimaging Clin N Am 24: 467-86, viii. doi: 10.1016/j.nic.2014.03.003
Knoll RM, Ishai R, Lubner RJ, Trakimas DR, Brodsky JR, Jung DH, Rauch SD, Nadol JB, Jr., Remenschneider AK, Kozin ED (2020) Peripheral Vestibular Organ Degeneration After Temporal Bone Fracture: A Human Otopathology Study. Laryngoscope 130: 752-760. doi: 10.1002/lary.28010
Kurihara YY, Fujikawa A, Tachizawa N, Takaya M, Ikeda H, Starkey J (2020) Temporal Bone Trauma: Typical CT and MRI Appearances and Important Points for Evaluation. Radiographics 40: 1148-1162. doi: 10.1148/rg.2020190023
Kwong Y, Yu D, Shah J (2012) Fracture mimics on temporal bone CT: a guide for the radiologist. AJR Am J Roentgenol 199: 428-34. doi: 10.2214/AJR.11.8012
Lantos JE, Leeman K, Weidman EK, Dean KE, Peng T, Pearlman AN (2019) Imaging of Temporal Bone Trauma: A Clinicoradiologic Perspective. Neuroimaging Clin N Am 29: 129-143. doi: 10.1016/j.nic.2018.08.005
Lyos AT, Marsh MA, Jenkins HA, Coker NJ (1995) Progressive hearing loss after transverse temporal bone fracture. Arch Otolaryngol Head Neck Surg 121: 795-9. doi: 10.1001/archotol.1995.01890070081017
Saraiya PV, Aygun N (2009) Temporal bone fractures. Emerg Radiol 16: 255-65. doi: 10.1007/s10140-008-0777-3
Suligavi SS, Saiyad SN, Doddamani SS, Mathri A (2022) Early Diagnosis of Hidden Hearing Loss Following Temporal Bone Fractures. Indian J Otolaryngol Head Neck Surg 74: 4336-4340. doi: 10.1007/s12070-021-02933-x
Swartz JD (2001) Temporal bone trauma. Semin Ultrasound CT MR 22: 219-28. doi: 10.1016/s0887-2171(01)90008-3
Wennmo C, Svensson C (1989) Temporal bone fractures. Vestibular and other related ear sequele. Acta Otolaryngol Suppl 468: 379-83.
Yoganandan N, Pintar FA (2004) Biomechanics of temporo-parietal skull fracture. Clin Biomech (Bristol, Avon) 19: 225-39. doi: 10.1016/j.clinbiomech.2003.12.014
![]()