By Marcello Cherchi, MD PhD
For patients
Hydrocephalus is sometimes colloquially referred to as “water on the brain.” It specifically refers to an excess of cerebrospinal fluid. This can happen at any age, and tends to have different causes in children than in adults. Common symptoms include headache, blurry vision and double vision. If there is strong reason to suspect hydrocephalus, then your doctor may consider checking a brain imaging study (such as a CT or MRI). Treatment of hydrocephalus depends on the underlying cause.
For clinicians
Overview
Hydrocephalus is the presence of excessive cerebrospinal fluid (CSF). Hydrocephalus is usually, though not always, associated with increased intracranial pressure and dilation of CSF ventricles. Hydrocephalus is usually classified as either obstructive or non-obstructive, and as congenital or acquired. The causes in children and adults tend to be different. Common presenting symptoms include headache, blurry vision, double vision, and sometimes cognitive changes. Ophthalmoscopic examination may show optic nerve head edema. Oculomotor examination may show a variety of abnormalities, the most common of which include trochlear nerve palsy. When hydrocephalus is clinically suspected, brain imaging is appropriate. Treatment depends on the underlying etiology.
Introduction
The term hydrocephalus refers to the presence of excessive cerebrospinal fluid (CSF). In most cases this is associated with an increase in intracerebral pressure (an exception being normal pressure hydrocephalus) and dilation of the CSF ventricles.
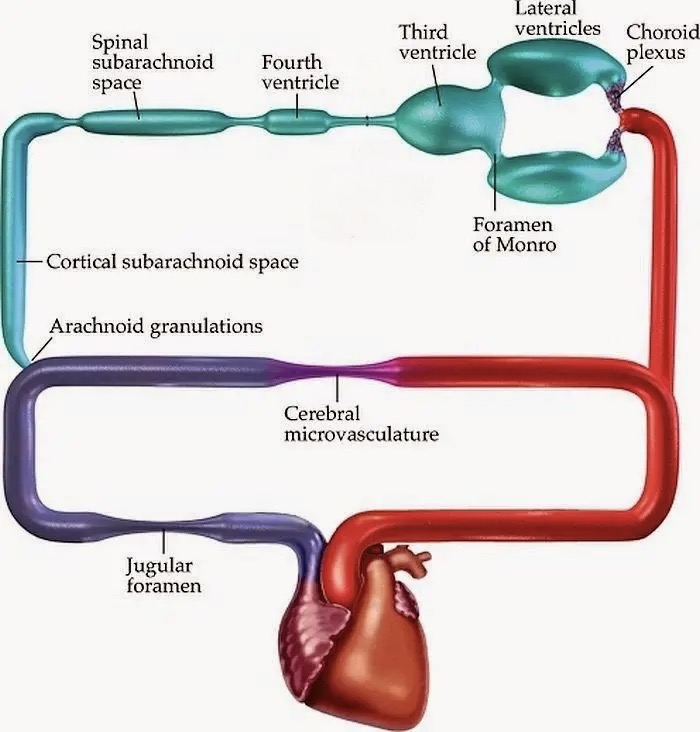
Cerebrospinal fluid is synthesized by the choroid plexus in the lateral ventricles, third and fourth ventricles. From the most proximal site of synthesis in the lateral ventricles, CSF flows through the interventricular foramina of Monro into the third ventricle, then through the cerebral aqueduct into the fourth ventricle. From there CSF passes through the medial aperture (foramen of Magendie) and lateral apertures (foramina of Luschka) of the fourth ventricle into the subarachnoid space at the skull base. CSF then flows through the subarachnoid space over the cerebral convexities and into the spinal canal. Finally, CSF is resorbed by the arachnoid villi (located in the superior sagittal sinus, intracranial venous sinuses, and around spinal nerve roots) into the blood stream. The movement of CSF is driven by the pressure waves from pulsation of the cerebral arteries (which expands the vascular component of intracerebral cerebral space and drives an equal volume of CSF to exit), propelling CSF along the pathway just described.
The Figure below is a schematic of CSF production (from serum), through the central nervous system, back into the bloodstream.
Pathophysiological mechanism of disease
A traditional classification of hydrocephalus distinguishes:
- Obstructive hydrocephalus (also called non-communicating hydrocephalus). This refers to a structural blockage somewhere between the site(s) of CSF production (at the choroid plexus in the lateral, third and fourth ventricles) and resorption (arachnoid granulations in the superior sagittal sinus, intracranial venous sinuses and around spinal nerve roots). For obstructive hydrocephalus the usual etiologies include tumors, intraventricular hemorrhage, vascular malformation and compression from edema.
- Non-obstructive hydrocephalus (also called communicating hydrocephalus). This refers to hydrocephalus from something other than obstructive (structural) causes, usually due to overproduction of CSF or impaired resorption of CSF, or both. In the “over-production of CSF” category is usually cited choroid plexus papilloma. In the “under-resorption of CSF” category the differential diagnosis includes damage to the arachnoid villi (such as from meningitis) or venous outflow obstruction (such as central venous sinus thrombosis).
A second dimension along which hydrocephalus is classified is whether it is congenital or acquired (Zhang, Williams et al. 2006). Etiologies of hydrocephalus in children and adults tend to be different.
Epidemiology
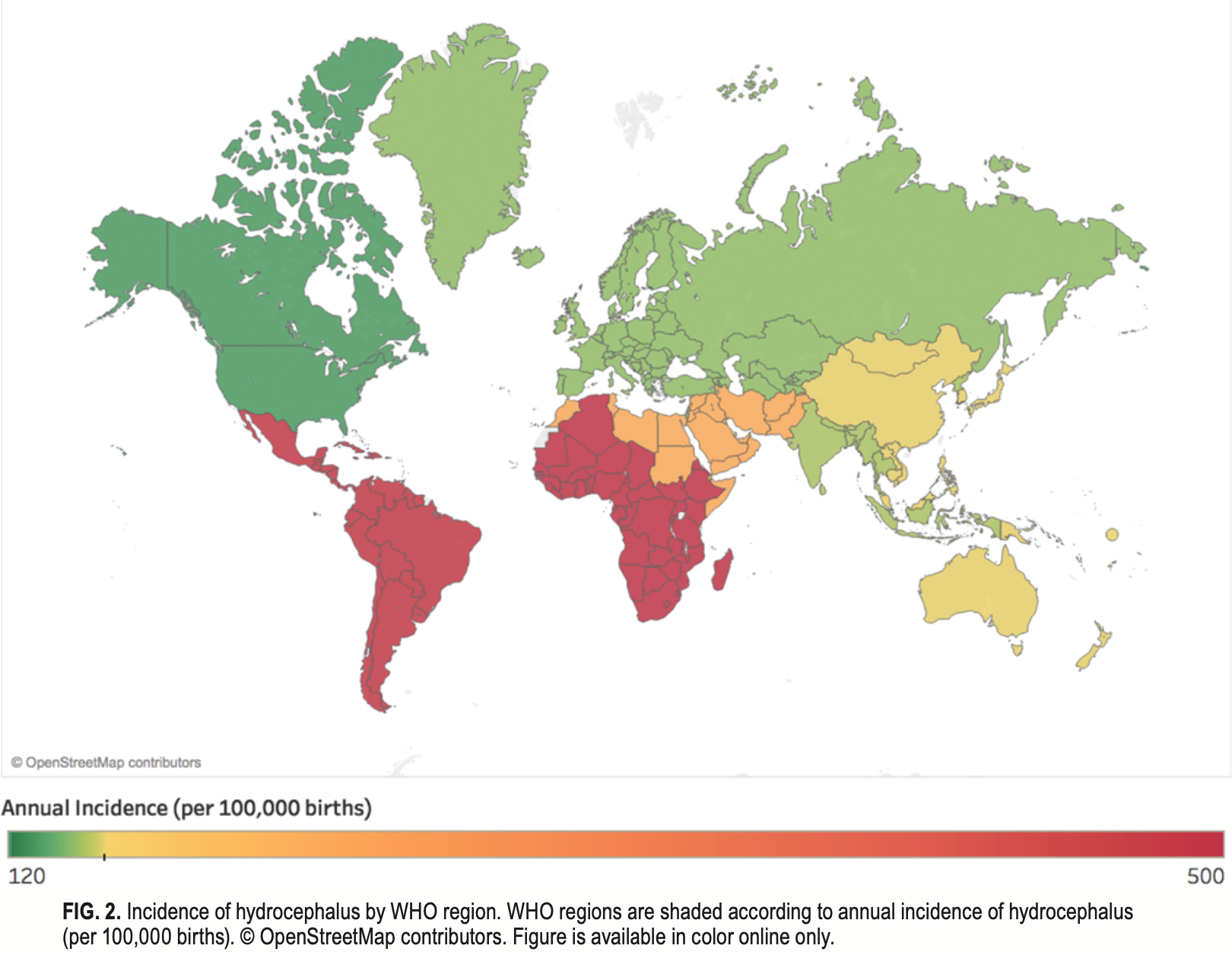
Hydrocephalus can occur at any age but is more common in infancy. Consequently the incidence depends on the age distribution of the population.
The Figure below, from Dewan and colleagues (Dewan, Rattani et al. 2018), shows the global annual incidence of hydrocephalus, which varies from 500 per 100,000 in low income regions, to 120 per 100,000 in middle and high income regions. There is a direct relationship between birth rate and incidence of hydrocephalus.
Genetics
A number of genes have been implicated in hydrocephalus (particularly congenital hydrocephalus) (Zhang, Williams et al. 2006, Garcia-Bonilla, McAllister et al. 2021), but the mechanism by which these genes bring about hydrocephalus remains unknown.
Clinical presentation
The clinical presentation of a patient with hydrocephalus will depend in part on the etiology of the hydrocephalus. However, in hydrocephalus from any cause, common symptoms include headache (presumably from traction on the innervated structures in the subarachnoid space), blurry vision (from optic nerve edema), diplopia (from various extraocular muscle palsies) and cognitive changes which can (if severe) include depressed level of consciousness (from herniation).
Physical examination
Physical examination of a patient with hydrocephalus will depend in part on the etiology of the hydrocephalus. From an otoneurological perspective we will omit from this discussion etiologies that would independently cause eye movement abnormalities, such as cerebellar hemorrhage (Pannu, Saroch et al. 2020).
Hydrocephalus often (though not always) causes optic disc edema which may be discernible on funduscopic examination.
Ocular motor examination
Many cases of hydrocephalus cause diplopia from strabismus. This usually happens secondary to trochlear nerve palsy, (Guy, Friedman et al. 1989, Mantopoulos, Hunter et al. 2011), but can also occur with palsies of the abducens nerve (Alver, Abuzayed et al. 2011) or ocular motor nerve (Cultrera, D’Andrea et al. 2009).
Some cases of hydrocephalus exert pressure on the quadrigeminal plate and thereby induce an upgaze palsy.
A variety of other ocular motor abnormalities have been reported in association with hydrocephalus (Gaston 1991, Lopponen, Sorri et al. 1992), including:
- Convergence nystagmus, or convergence-retraction nystagmus (Chattha and Delong 1975, Sato, Maehara et al. 1983, Keane 1985, Maroulis, Halmagyi et al. 2008, Hashizume, Watanabe et al. 2011), in isolation or as part of pretectal syndrome (Keane 1990).
- Spontaneous down beat nystagmus (Phadke, Hern et al. 1981).
- Opsoclonus (Shetty and Rosman 1972).
- Abnormal optokinetic responses (Suzuki, Harada et al. 1985).
- Positional nystagmus (Sweeney, Hahn et al. 1980, Power, Murray et al. 2019).
- Pseudobobbing (Keane 1985).
- Skew deviation (Moguel-Ancheita, Castellanos-Perez Bolde et al. 2009) not due to extraocular muscle palsy.
- Spontaneous up beat nystagmus (Kim, Yoon et al. 2006).
- Wall-eyed bilateral internuclear ophthalmoplegia (WEBINO) (Keereman, Platteau et al. 2018)
Many patients with hydrocephalus, especially in the early stages, have normal eye movements. Consequently, the diagnosis of hydrocephalus does not depend on the presence of ocular motor abnormalities.
Imaging
When hydrocephalus is clinically suspected, brain imaging is appropriate.
Treatment
The treatment of hydrocephalus depends on the underlying etiology.
Prognosis
Hydrocephalus, if presenting acutely and progressing rapidly, runs the risk of various types of brain herniation (subfalcine, central transtentorial, uncal transtentorial, upward cerebellar, downward cerebellar tonsillar) depending on the etiology of hydrocephalus. Brain herniation is life-threatening; these patients require emergent neurosurgical evaluation and are usually observed in a neuro-intensive care unit.
References
Alver I, Abuzayed B, Kafadar AM, Muhammedrezai S, Sanus GZ, Akar Z (2011) Primary fourth ventricular meningioma: case report and review of the literature. Turk Neurosurg 21: 249-53. doi: 10.5137/1019-5149.JTN.2869-09.0
Chattha AS, Delong GR (1975) Sylvian aqueduct syndrome as a sign of acute obstructive hydrocephalus in children. J Neurol Neurosurg Psychiatry 38: 288-96. doi: 10.1136/jnnp.38.3.288
Cultrera F, D’Andrea M, Battaglia R, Chieregato A (2009) Unilateral oculomotor nerve palsy: unusual sign of hydrocephalus. J Neurosurg Sci 53: 67-70.
Dewan MC, Rattani A, Mekary R, Glancz LJ, Yunusa I, Baticulon RE, Fieggen G, Wellons JC, Park KB, Warf BC (2018) Global hydrocephalus epidemiology and incidence: systematic review and meta-analysis. J Neurosurg: 1-15. doi: 10.3171/2017.10.JNS17439
Garcia-Bonilla M, McAllister JP, Limbrick DD (2021) Genetics and Molecular Pathogenesis of Human Hydrocephalus. Neurol India 69: S268-S274. doi: 10.4103/0028-3886.332249
Gaston H (1991) Ophthalmic complications of spina bifida and hydrocephalus. Eye (Lond) 5 ( Pt 3): 279-90. doi: 10.1038/eye.1991.44
Guy JR, Friedman WF, Mickle JP (1989) Bilateral trochlear nerve paresis in hydrocephalus. J Clin Neuroophthalmol 9: 105-11.
Hashizume A, Watanabe H, Matsuo K, Katsuno M, Tanaka F, Nagatani T, Sobue G (2011) Endoscopic third ventriculotomy improves parkinsonism following a ventriculo-peritoneal shunt in a patient with non-communicating hydrocephalus secondary to idiopathic aqueduct stenosis. J Neurol Sci 309: 148-50. doi: 10.1016/j.jns.2011.07.025
Keane JR (1985) Pretectal pseudobobbing. Five patients with ‘V’-pattern convergence nystagmus. Arch Neurol 42: 592-4. doi: 10.1001/archneur.1985.04060060098017
Keane JR (1990) The pretectal syndrome: 206 patients. Neurology 40: 684-90. doi: 10.1212/wnl.40.4.684
Keereman V, Platteau E, Crevits L, Algoed L (2018) Wall-eyed Bilateral Internuclear Ophthalmoplegia (WEBINO) in a Patient With Idiopathic Intracranial Hypertension. Neurologist 23: 157-159. doi: 10.1097/NRL.0000000000000192
Kim JS, Yoon B, Choi KD, Oh SY, Park SH, Kim BK (2006) Upbeat nystagmus: clinicoanatomical correlations in 15 patients. J Clin Neurol 2: 58-65. doi: 10.3988/jcn.2006.2.1.58
Lopponen H, Sorri M, Serlo W, von Wendt L (1992) ENG findings of shunt-treated hydrocephalus in children. Int J Pediatr Otorhinolaryngol 23: 35-44. doi: 10.1016/0165-5876(92)90077-3
Mantopoulos D, Hunter DG, Cestari DM (2011) Isolated bilateral fourth cranial nerve palsies as the presenting sign of hydrocephalus. Case Rep Ophthalmol 2: 211-4. doi: 10.1159/000330336
Maroulis H, Halmagyi GM, Heard R, Cook RJ (2008) Sylvian aqueduct syndrome with slit ventricles in shunted hydrocephalus due to adult aqueduct stenosis. J Neurosurg 109: 939-43. doi: 10.3171/JNS/2008/109/11/0939
Moguel-Ancheita S, Castellanos-Perez Bolde CG, Orozco-Gomez LP (2009) Skew deviation. Strabismological diagnosis and treatment alternatives. Cir Cir 77: 267-73; 249-55.
Pannu AK, Saroch A, Sharma N (2020) Intracerebellar Hemorrhage in a Young Adult. Indian J Crit Care Med 24: 69-70. doi: 10.5005/jp-journals-10071-23330
Phadke JG, Hern JE, Blaiklock CT (1981) Downbeat nystagmus–a false localising sign due to communicating hydrocephalus. J Neurol Neurosurg Psychiatry 44: 459. doi: 10.1136/jnnp.44.5.459
Power L, Murray K, Bullus K, Drummond KJ, Trost N, Szmulewicz DJ (2019) Central Conditions Mimicking Benign Paroxysmal Positional Vertigo: A Case Series. J Neurol Phys Ther 43: 186-191. doi: 10.1097/NPT.0000000000000276
Sato Y, Maehara F, Utsunomiya H, Hayashi T, Moritaka K, Kaji M (1983) Convergence and retraction nystagmus in hydrocephalus due to shunt malfunction. Kurume Med J 30: 125-8. doi: 10.2739/kurumemedj.30.125
Shetty T, Rosman NP (1972) Opsoclonus in hydrocephalus. Arch Ophthalmol 88: 585-9. doi: 10.1001/archopht.1972.01000030587001
Suzuki M, Harada Y, Ishida M, Wada H, Ohta M, Sakoda K, Uozumi T (1985) Aqueductal stenosis–results of vestibular function tests. J Laryngol Otol 99: 151-61. doi: 10.1017/s0022215100096444
Sweeney PJ, Hahn JF, McHenry MC, Mitsumoto H (1980) Mucormycosis presenting as positional nystagmus and hydrocephalus. Case report. J Neurosurg 52: 270-2. doi: 10.3171/jns.1980.52.2.0270
Zhang J, Williams MA, Rigamonti D (2006) Genetics of human hydrocephalus. J Neurol 253: 1255-66. doi: 10.1007/s00415-006-0245-5
![]()