By Marcello Cherchi, MD PhD
For patients
Benign paroxysmal positional vertigo (BPPV) is the most common cause of disequilibrium overall. This disease happens when tiny crystals in the inner ear break loose and get into other parts of the inner ear (where they do not belong). Patients with BPPV usually have episodes of spinning disequilibrium triggered by various head movements, such as rolling over in bed, or tilting the head backwards or forwards. Your doctor or vestibular physical therapist can often can figure out if you have BPPV by examining your eye movements, though sometimes they may need to examine you several times to “catch” these eye movements. BPPV is treated with a variety of physical therapy maneuvers that your therapist can sometimes teach you. BPPV is not treated with medication or surgery. Even when treated well, BPPV often happens again, and there is not yet any known way of preventing this.
For clinicians
Practical summary
Benign paroxysmal positional vertigo (BPPV) is the most common cause of disequilibrium over the lifespan. The mechanism of BPPV is that otoliths (that normally reside in the utricle) break loose and enter the semicircular canals, where their influence on endolymphatic fluid dynamics results in inappropriate stimulation of the ampullar maculae, thereby provoking both nystagmus and symptoms. BPPV usually presents with positionally-triggered episodes of disequilibrium that usually, though not always, have a spinning quality. BPPV can occur at any age, though it is less common before the age of about 40 years, after which its incidence increases exponentially. Besides age, additional risk factors include a history of migraine, other ear disease (e.g., vestibular neuritis, labyrinthitis, Ménière’s disease), and perhaps vitamin D deficiency. A diagnosis of BPPV is secured when an examiner observes a pattern of eye movements; the specific pattern of eye movements depends on which canal (or combination of canals) is affected by BPPV. Since BPPV is by its nature paroxysmal, these eye movements may not always be evident on examination. The diagnostic eye movements may also be obfuscated by vestibular suppressant medications. Treatment of BPPV consists of appropriately targeted canalith repositioning maneuvers; the specific maneuver will depend on which canal (or combination of canals) is affected. The canalith repositioning maneuvers often have to be repeated. Most literature suggests that sleeping upright (after physical therapy treatment) does not affect treatment outcome. Medications and surgery play no significant role in management of BPPV. The natural history of BPPV is one of recurrence, and there is not yet any firmly established prophylactic intervention.
§1: BPPV overview
§1.1: What is BPPV?
Benign paroxysmal positional vertigo (BPPV) is an inner ear disorder that usually causes positionally-triggered episodes of dizziness/imbalance. It is among the most frequently encountered diseases in clinics specializing in evaluating dizzy patients.
In 1920 Robert Bárány (Bárány 1920) described a case of a young woman who had been suffering from vertiginous episodes triggered by lying on her right side. Numerous similar cases were described subsequently, and in 1952 Margaret Ruth Dix and Charles Skinner Hallpike (Dix and Hallpike 1952a, b)described their own cases of “positional nystagmus” (the term nystagmus refers to “jumping of the eyes”), noting that symptoms (and simultaneous nystagmus) were induced, “by a critical position of the head in space.”
The phrase “benign paroxysmal positional vertigo” is very entrenched in the literature, and unlikely to change soon. However, Strupp and colleagues (Strupp et al. 2026) have reasonably argued that this nomenclature is misleading because it implies benignity (despite the significant impairment it sometimes causes) and it fails to acknowledge the peripheral (otologic) etiology of the diagnosis. For these reasons, Strupp and colleagues instead suggest the tern “peripheral paroxysmal positional vertigo (PPPV).”
§1.2: When should one suspect BPPV?
In the majority of cases, BPPV presents as positionally-triggered episodes of disequilibrium that patients usually experience as a spinning sensation (sometimes associated with nausea) that can last seconds to minutes, though can be followed by many minutes of unsteadiness. The symptoms can be re-triggered when the patient assumes the same position.
In some instances (usually lateral semicircular canal BPPV, which will be discussed in greater detail below) the sensation of disequilibrium is more vague, and may be experienced as a “rocking,” “tilting” or “swaying.” Despite the fact that the semicircular canals mediate sensations of angular acceleration, BPPV can in some cases cause sensation of linear motion as well (Choi et al. 2021).
If a patient is experiencing these sensations, then BPPV is a reasonable possibility. However, in order to be confident about the diagnosis, a clinician needs to examine a patient’s eye movements, as will be discussed below.
§1.3: What is the cause of BPPV?
BPPV is the result of otoliths (“crystals” in the inner ear) coming loose from their normal place in the inner ear (the saccule and the utricle) and entering an incorrect place (the semicircular canals) in the inner ear. The movement of the otoliths results in stimulation of motion sensors, which in turn provokes a sensation of movement.
Notice that in order for this disease to manifest, two distinct events need to occur. First, the otoliths need to break loose; this appears to occur spontaneously, and there is very little a person can do to physically to break the otoliths loose. Second, the otoliths need to get into an incorrect part of the ear; this simply happens when the head is put in certain orientations with respect to gravity.
Thus, when a person goes to the hairdresser, extends her neck over the edge of the washbasin, becomes dizzy and then gets diagnosed with BPPV, it is easy to fall prey to the misapprehension that “bending my head backwards broke the crystals loose and caused BPPV,” but that is probably not true; it is far more likely that the otoliths were already loose before she went to the hairdresser, and once they were loose, inclining the head backwards permitted those (already loose) otoliths to enter one of the semicircular canals, thereby provoking symptoms.
Much of the information on the internet gives the erroneous impression that BPPV is a matter of there being “one ball bearing that is loose,” but actually this is more of a “grains of sand” issue — hence BPPV is a matter of degree, and can be present to a greater or lesser extent.
§1.4: Epidemiology of BPPV
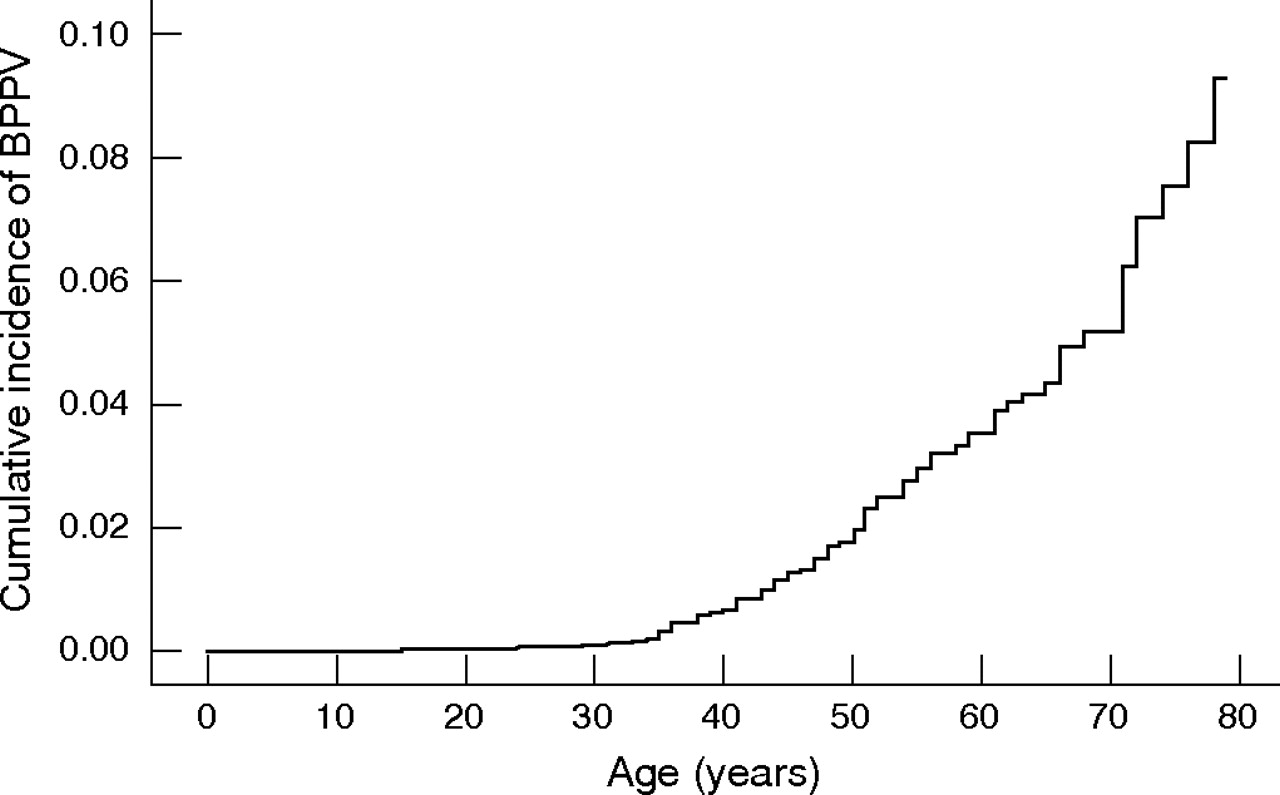
BPPV is the most common cause of dizziness over the lifespan (Nedzelski, Barber, McIlmoyl 1986; Neuhauser 2007; Parnes, Agrawal, Atlas 2003). It is less common before the age of about 40 years, after which its incidence increases exponentially (von Brevern et al. 2007), as shown in the Figure below.
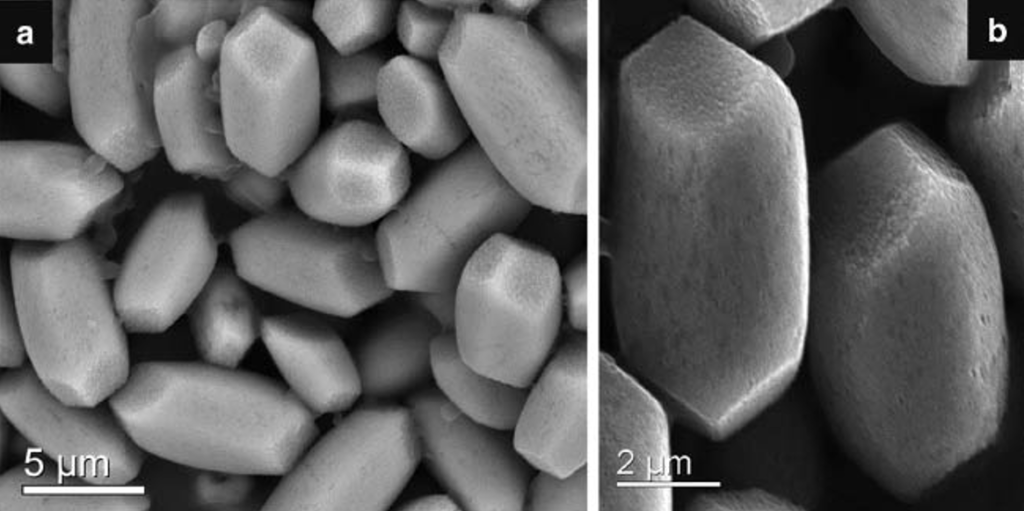
The recognition of this relationship led to the idea that BPPV is somehow due to “wear and tear” on the inner ear. Electron micrographs actually support this idea. The Figure below shows otoconia in a normal, healthy individual (Kniep 2015).
As a person ages, even if they are otherwise healthy, the otoconia begin to fragment, as shown in the Figure below (Walther and Westhofen 2007).
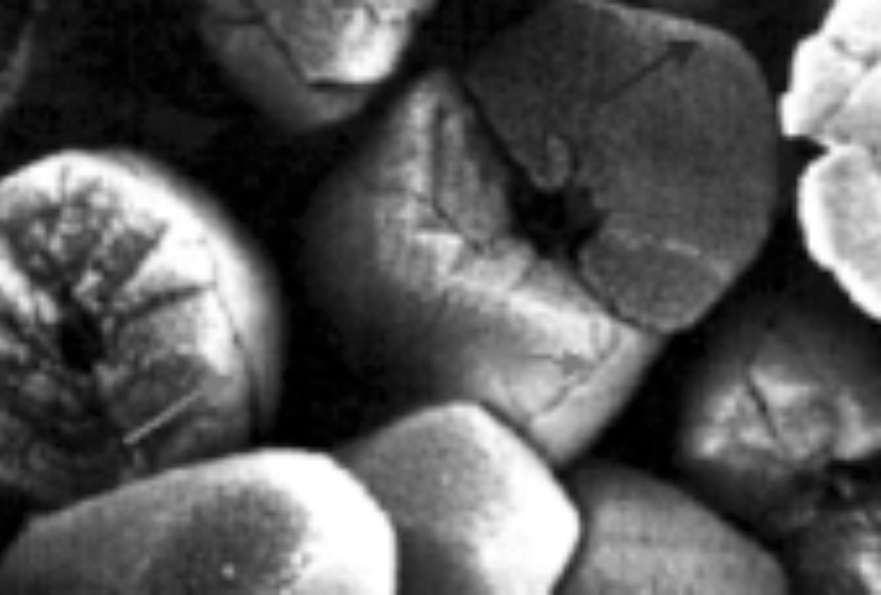
Given this deterioration of otoliths, it is not hard to imagine fragments of otoliths breaking loose.
§1.5: Risk factors for BPPV
Most cases of BPPV appear to occur without any discernible trigger — specifically, there is usually nothing in the patient’s history that would explain why the otoliths “broke loose.”
Probably the single most important risk factor for BPPV is a history of a prior episode of BPPV. This is because BPPV has a tendency to recur (see below).
Since BPPV occurs more frequently with increasing age (see above), older age is also considered a “risk factor” for BPPV.
There are a few other factors that appear to increase the risk of BPPV, though the literature about these is mixed. A history of migraine appears to increase the risk of BPPV (Ishiyama, Jacobson, Baloh 2000; Kim et al. 2019). Low bone density (Jeong et al. 2009) and vitamin D deficiency (Chen et al. 2020) may increase the risk of BPPV. Finally, the risk of BPPV appears to be increased when a patient has a history of other ear diseases (Lee et al. 2010), such as vestibular neuritis (Balatsouras et al. 2014), labyrinthitis (Baloh, Honrubia, Jacobson 1987) and Ménière’s disease (Kutlubaev, Xu, Hornibrook 2019).
BPPV can occur following various dental procedures (Chang et al. 2016) such as dental extractions (Chiarella et al. 2008), placement of dental implants (Bennardo et al. 2022; Crespi et al. 2013, 2014; Galli et al. 2004; Kaplan et al. 2003; Penarrocha-Diago et al. 2008; Rodriguez Gutierrez and Rodriguez Gomez 2007; Wanner et al. 2013), removal of dental implants (Messina and Marini 2018) and other procedures (Brauer 2009).
BPPV can also occur after various maxillofacial surgeries, such as nasal septoplasty (Kansu et al. 2015) and sinus floor elevation (Akcay et al. 2016; Crespi et al. 2012; Damsaz et al. 2024; Giannini et al. 2015; Hsu et al. 2022; Molina et al. 2022; Pjetursson and Lang 2014; Reddy et al. 2015; Sammartino et al. 2011; Stacchi et al. 2022; Su et al. 2008; Vernamonte et al. 2011).
The literature provides conflicting data on the relationship between head trauma and BPPV. For example, some literature suggests that BPPV following head trauma is less responsive to treatment (Babac et al. 2014; Balatsouras et al. 2017; Pisani et al. 2015); in contrast, large case series (Luryi et al. 2019) and meta-analyses (Aron et al. 2015) concluded that the available evidence does not show any difference in treatment responsiveness/outcomes between traumatic and non-traumatic BPPV. There is modest literature suggesting that bilateral posterior semicircular canal involvement (Katsarkas 1999) or (unilateral) anterior semicircular canal involvement (Dlugaiczyk et al. 2011; Jackson et al. 2007) are more common following head trauma. From a practical medical perspective these considerations are irrelevant in the sense that, if a patient has manifest BPPV on examination, treatment should be considered, irrespective of prior history.
§1.6: Genetics
There is no clear genetic predisposition specifically for BPPV, though some have been implicated. For example:
- LOXL1 (lysyl oxidate-like 1 on chromosome 15q24.1, see OMIM 153456) (Deng et al. 2020).
- PCDHGA10 (protocadherin-gamma subfamily A10 on chromosome 5q31.3, see OMIM 606297) (Xu et al. 2021)
- Some genetic conditions responsible for other ear diseases may increase the risk of BPPV. For example, the STRC gene on chromosome 15q15.3 encodes for the protein of stereocilin (OMIM 606440); mutations in this gene cause DFNB16 (autosomal recessive deafness type 16, OMIM 603720). There are reports of STRC mutations associated with recurrent BPPV (Achard et al. 2023a; Achard et al. 2023b).
Until there is further clarification, genetic testing does not usually play a role in the workup of BPPV.
§2: Diagnosing BPPV
§2.1: How is BPPV diagnosed?
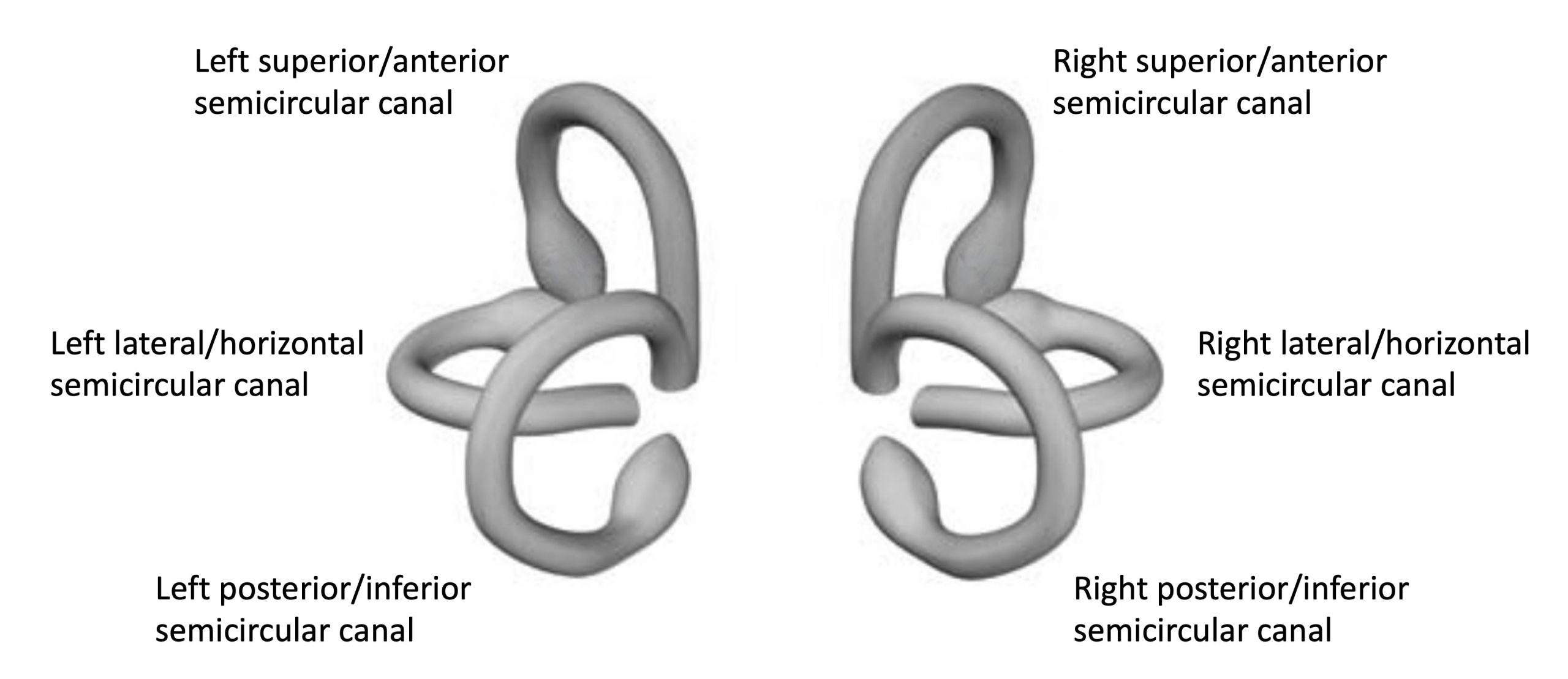
BPPV can be suspected from the clinical history, but can only be confirmed by observation of a pattern of eye movements (von Brevern et al. 2015). The specific pattern of eye movements depends on which semicircular canal, or combination of the six semicircular canals, is affected by BPPV (see Figure, below). The eye movements consist of various combinations of nystagmus; nystagmus refers to a repetitive pattern in which there is a slow eye movement in a given direction, followed by a quick eye movement in the opposite direction, and then the cycle repeats.
Note that the magnitude of the nystagmus does not necessarily correspond to the degree of symptoms (Karababa et al. 2025).
§2.2: Are there tests for BPPV?
Observation of eye movements IS THE TEST for confirming BPPV (von Brevern, Bertholon et al. 2015, Bhattacharyya, Gubbels et al. 2017, von Brevern, Bertholon et al. 2017).
In a patient who is already known to have BPPV, there may be some circumstances in which studying their inner ear function is appropriate. If a patient appears not to be responding well to appropriately targeted treatment, many clinicians may consider checking tests of inner ear function in order to assess whether the ears have been damaged by some other disease process, which in turn might have rendered the patient more vulnerable to BPPV. For example, there is emerging evidence that assessment of vestibular evoked myogenic potentials may be useful in this regard (Hong, Park et al. 2008, Yang, Kim et al. 2008, Korres, Gkoritsa et al. 2011, Lee, Park et al. 2013, Yetiser, Ince et al. 2014, Hoseinabadi, Pourbakht et al. 2016, Singh and Apeksha 2016, Xu, Liang et al. 2016, Oya, Imai et al. 2019, Scarpa, Gioacchini et al. 2019).
§2.3: Someone examined me and did not “see” BPPV, so do I really have it?
There are several reasons why an individual who truly has BPPV may not exhibit the associated eye movements on a particular examination.
The first reason why the diagnostic eye movements might not be seen in a person who truly has BPPV has to do with the behavior of the disease itself. BPPV is an episodic problem, which is why it has the word “paroxysmal” in its title. Because of this pattern, the diagnostic eye movements will not necessarily be present every time an examiner looks for them. As an example, the Dix-Hallpike maneuver is considered the “gold standard” for the diagnosis of posterior semicircular canal BPPV (Bhattacharyya, Gubbels et al. 2017); however, the maneuver has a reported specificity of 71% (Lopez-Escamez, Lopez-Nevot et al. 2000) and negative predictive value of 52% (Hanley and O’Dowd 2002), meaning that a “negative” Dix-Hallpike maneuver does not entirely exclude the presence of posterior canal BPPV; for this reason, if a patient’s history is suggestive of BPPV yet her examination does not “show it,” it is reasonable to re-examine the patient at some interval. That being said, the more frequently one looks for the abnormal eye movements and fails to detect them, the more skeptical one becomes about the diagnosis.
The second reason why the diagnostic eye movements might not be seen in a person who truly has BPPV is that the examiner may be relying on an insufficiently sensitive method of detection; for example, the examiner may not using infrared video Frenzel oculography (Frenzel 1956; Levo, Aalto, Petteri Hirvonen 2004). If a clinician is only observing a patient’s eye movements “face-to-face,” or only using Fresnel lenses (Fresnel 1822; Strupp et al. 2014), then some degree of vision is available to the patient; when vision is available, the brain is hard-wired to make a person visually fixate on targets, and such fixation can suppress a variety of eye movement abnormalities (Baloh et al. 1977; Chambers and Gresty 1982; Gauthier and Vercher 1990; Gizzi and Harper 2003; Hart 1967; Hirvonen, Juhola, Aalto 2012; Karlsen, Goetzinger, Hassanein 1980; Katsarkas and Kirkham 1982; Molnar and Torok 1974; Sokolovski 1966), including many of the eye movement abnormalities that are diagnostically helpful.
The third reason why the diagnostic eye movements might not be seen in a person who truly has BPPV is that the abnormal eye movements (which would otherwise be present) can be suppressed by certain medications, such as vestibular suppressants (e.g., meclizine, dimenhydrinate), or benzodiazepines.
It should also be noted that if a patient suspected of having BPPV has repeatedly normal exams (despite an adequate examination technique, and despite being off vestibular suppressant medications), then the suspected diagnosis may be incorrect. We discuss this further below.
§2.4: In a patient with BPPV is it necessary to get brain imaging?
If a person’s clinical history and eye movements are compatible with BPPV, and if her physical examination is otherwise normal, then brain imaging is usually unnecessary (Bhattacharyya, Gubbels et al. 2017).
§3: Subtypes of BPPV
Although we have been speaking of a “diagnosis of BPPV,” there are several subtypes of this disease, depending on the specific semicircular canal or combination of semicircular canals involved.
When BPPV affects a single canal in a single ear, the statistics of involvement are (Fife 2012):
- Posterior canal: 81 – 89% of cases
- Lateral canal: 8 – 17% of cases
- Anterior canal: 1 – 3% of cases
These statistics are not uncontroversial; for instance, Bhandari and colleagues (Bhandari, Bhandari et al. 2023) report a very different distribution of cases: out of 3,975 BPPV patients they identified 47.8% had posterior canal involvement, 46.3% had lateral canal involvement, and 0.7% had anterior canal involvement — in other words, they found that lateral canal involvement comprised a significantly higher proportion of cases than in other studies.
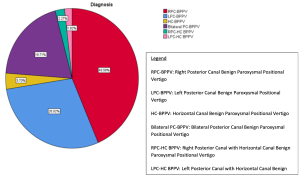
BPPV can affect combinations of canals (Tomaz et al. 2009). The data in the Figure below, from Chua Wei De and colleagues (Chua Wei De et al. 2020), shows a pie chart depicting the relative proportions of canals and combinations of canals affected by BPPV in a population of 1542 patients.
The treatment maneuvers for each type of BPPV are discussed elsewhere.
§4: Treatment for BPPV
§4.1: Do I need to treat BPPV?
The management of BPPV is “symptom-driven,” meaning that if symptoms are infrequent and mild, some patients reasonably elect to refrain from treatment, since spontaneous resolution (i.e., without treatment) can occur. If one initially elects to refrain from treatment but then the symptoms become more aggressive, then treatment can be initiated; it is never “too late” to treat BPPV.
§4.2: Treatment for BPPV: Physical therapy
Appropriately targeted vestibular rehabilitation therapy is firmly established as the standard of care for BPPV (Bhattacharyya et al. 2017). The particular series of physical therapy maneuvers is chosen based on which semicircular canal, or combination of semicircular canals, is involved.
§4.2.1: Mechanism of physical therapy
Note that the physical therapy exercises do not “put the crystals back in place.” Rather, by moving the head through certain positions, these maneuvers exploit gravity to “coax” the loose otoliths out of the semicircular canals, and into parts of the ear where they have a higher chance of getting resorbed.
Note that even when BPPV has been correctly diagnosed, and even when the appropriately targeted treatment maneuver has been initiated, the response to therapy may be somewhat uneven; observing symptoms day-to-day, it may appear that on a given day the patient feels worse than the previous day; however, when observing symptoms over a longer span of time (several days in a row), the overall trajectoryshould be one of improvement. If the overall trajectory of symptoms is one of improvement (no matter how slow it seems), then the patient is likely pursuing the correct treatment.
In contrast, if while performing a given exercise the patient finds that symptoms are growing consistently worse with each day of treatment, for several days in a row, then this raises the possibility that the patient has suffered a “canal conversion” (in which the otoliths have exited one semicircular canal but entered a different semicircular canal; see the section below entitled, “Why is my treatment for BPPV unsuccessful?”). In this circumstance the patient should refrain from further self-treatment, and seek treatment by a physical therapist or physician so that they can examine the patient’s eye movements.
§4.2.2: Why do the physical therapy treatment maneuvers need to be repeated?
The various exercises do help maneuver the loose otoliths into a part of the ear where they have a better chance of getting resorbed, but the exercises do not cause resorption instantaneously, they do not immediately dissolve the crystals, and they do not “glue the crystals back into place.” The crystals are still there, and while a few of them will get resorbed shortly after the exercises are performed, the remaining otoliths are still loose, and in the course of daily activities and head movements, some of those loose crystals will get back into places where they don’t belong (the semicircular canals), where they will still be capable of provoking symptoms.
Therefore, where patients get the most “mileage” out of the treatment exercises is by repeating them over time. Thus, doing the appropriately targeted exercises 30 times in one night is actually less effective than doing those exercises 3 times per day over 10 days.
§4.2.3: Do I need to sleep upright after doing the treatment maneuvers?
In posterior semicircular canal BPPV, lying supine and rolling over in bed often provoke symptoms, so it is reasonable to inquire whether remaining upright, or at least remaining in a partially reclined position (between completely upright and completely supine) might help. The short answer is that remaining upright may avert symptom provocation, but merely remaining upright does not in itself treat BPPV.
A related question is whether sleeping upright improves the efficacy of the various treatment maneuvers for BPPV. Most literature on this topic concludes that sleeping upright does not improve treatment outcomes for BPPV (Casqueiro, Ayala, Monedero 2008; De Stefano et al. 2011; Devaiah and Andreoli 2010; Fyrmpas et al. 2009; Gordon and Gadoth 2004; Moon et al. 2005; Mostafa, Youssef, Hamad 2013; Nuti, Nati, Passali 2000; Roberts et al. 2005; Simoceli, Bittar, Greters 2005). A few studies suggest that sleeping upright may be helpful (Cakir et al. 2006; McGinnis et al. 2009), while other studies simply conclude that further research is needed on this topic (Papacharalampous et al. 2012).
§4.3: Treatment for BPPV: Medication
Medications such as vestibular suppressants (meclizine, dimenhydrinate) and benzodiazepines (clonazepam, diazepam) are sometimes prescribed, but their role in treating BPPV is very limited, and guidelines generally recommend against their use (Bhattacharyya et al. 2017).
It must be kept in mind that these medications may succeed in “dampening” the sensation of dizziness, but they do not actually treat the underlying cause of BPPV — specifically, they do not dissolve otoliths or reattach them in their proper place.
These medications also pose several problems. The first is that by suppressing symptoms, it makes it more difficult to assess whether the disease causing those symptoms is actually improving — in other words, it may be hard to tell whether a given treatment maneuver is effective. The second problem is that these medications also suppress eye movements, thereby making it difficult to verify the diagnosis and monitor treatment responsiveness. The third problem is that these medications tend to be soporific (cause sleepiness).
Despite the discussion above, some investigators have made the case that medication may serve an adjunctive role to physical therapy (Chen et al. 2023). We agree that in selected cases this may be appropriate; for example, if a patient’s diagnosis of BPPV is secure and confidently localized (meaning that the involved canal is known and has been consistent) but the patient is having difficulty tolerating canalith repositioning maneuvers (e.g., due to significant nausea and vomiting) and thus is refraining from treatment, then premedicating with a vestibular suppressant may make it feasible for the patient to engage in appropriately targeted physical therapy.
§4.4: Treatment for BPPV: Surgery
A variety of essentially destructive procedures have been attempted by otolaryngologists in the management of BPPV.
Of the surgical procedures attempted for management of BPPV the most common is “canal plugging,” first reported by Lorne Parnes and Joseph McClure (Parnes and McClure 1990). In this procedure the surgeon fills the semicircular canal affected by BPPV with either bone pâté or a synthetic substance. The logic of this procedure is that plugging the affected canal “silences” it, because otoliths can no longer enter it. Subsequent studies (Shaia et al. 2006) reported impressive success with this procedure, but it was soon realized (Kisilevsky et al. 2009) that potential complications of the procedure included hearing loss, vestibular deficits on objective testing, and even continued dizziness. The continued dizziness was particularly concerning, since that was the symptom the procedure was intended to treat. Among other problems, it was eventually recognized (Luryi et al. 2018b) that although plugging one canal might “silence” that canal, there remain five other semicircular canals that are still susceptible to developing BPPV.
A less commonly attempted surgical procedure for management of BPPV is cutting the nerve that transmits balance signals from the ear to the brain (which procedure is called “vestibular neurectomy”) or, if possible, cutting just the part of that nerve that transmits balance signals from the affected canal (which procedure is called “singular neurectomy” (Gacek 1978)). While the latter procedure (singular neurectomy) appeared promising and minimally destructive, it also turned out to be technically challenging, and few surgeons attempted it.
Taking these factors into consideration, we generally do not recommend surgery as a treatment for patients with BPPV.
§4.5: Why is my treatment for BPPV unsuccessful?
There are several reasons why treatment for BPPV may be unsuccessful.
The first is that the specific case of BPPV may be very aggressive. This likely corresponds to a situation in which a very large number of otoliths have broken loose, thereby requiring more extended treatment before resorption is complete.
The second reason by treatment of BPPV may be unsuccessful is what is termed a “canal conversion” (Anagnostou, Stamboulis, Kararizou 2014; Babic et al. 2014; Dispenza et al. 2015; Foster, Zaccaro, Strong 2012; Lee et al. 2019; Lin et al. 2012; Park et al. 2013). Since all parts of the inner ear are connected, there is nothing to prevent otoliths from exiting one incorrect place and migrating to a different incorrect place — in other words, leaving one semicircular canal and entering another one. This is a problem because the semicircular canals are arranged in different orientations, so a treatment maneuver directed at one semicircular canal will be ineffective as treatment for a different semicircular canal. Clinically this may be evident if a patient who had been improving with treatment suddenly starts to deteriorate.
The third reason why treatment of BPPV may be unsuccessful is that multiple semicircular canals may be involved, and this situation is generally more difficult to treat. In some cases, at the time of diagnosis it is recognized that multiple canals are involved. In other cases, a patient may begin with involvement of only one canal, but subsequently develop involvement of multiple canals.
A fourth reason why treatment of BPPV may be unsuccessful is that the patient has not only BPPV, but some other vertiginous disease as well. This may become evident if, during the course of treatment for BPPV, a patient’s eye movements normalize (in other words, there nystagmus that is diagnostic of BPPV is no longer present on several sequential examinations), yet the patient still complains of symptoms. In this circumstance it is reasonable to suspect that an additional disease may be at play.
A fifth reason why treatment of BPPV may be unsuccessful is that the patient actually does not have BPPV. Sometimes, even when practitioners are working in good faith and to the best of their abilities, a diagnosis of BPPV may simply be incorrect.
§4.6: Can recurrences of BPPV be prevented?
Since the treatment for BPPV is a specific series of maneuvers (described earlier), many patients reasonably ask whether they should continue doing these maneuvers in order to “ward off” future episodes. This approach has been studied, and found to be ineffective (Helminski, Janssen, Hain 2008). The maneuvers only work when BPPV is “active” (i.e., when symptoms are present). When symptoms are absent, that is because there are no more loose otoliths, and in this “quiescent” state, there is nothing for the maneuvers to “act on.”
The observation that vitamin D deficiency may increase the risk of BPPV (Chen et al. 2020) leads to the question of whether supplementation of vitamin D might reduce the risk. There is emerging evidence that, after a first episode of BPPV, taking vitamin D and perhaps calcium may reduce the likelihood of recurrence of BPPV (Jeong, Lee, Kim 2020). For instance, a randomized controlled trial (Jeong et al. 2020) reported that supplementation with vitamin D 400 I.U. and calcium carbonate 500 mg twice per day reduces the annual recurrence rate of BPPV. Note that increasing one’s level of vitamin D (even without supplementing additional calcium) may increase serum calcium concentrations, which at least in theory can increase the risk of developing kidney stones (Letavernier and Daudon 2018), though it is unclear whether this increased risk is clinically meaningful; one might think that vitamin D supplementation should perhaps be avoided in persons who already have a history of kidney stone formation, but this does not seem to be borne out by the evidence (Ganji, Shafii, Hakemi 2019); if you are considering supplementing your vitamin D intake (with or without calcium supplementation), please consult your primary care physician first.
§5: Residual disequilibrium following apparently successful treatment of BPPV
It is well documented that some patients with BPPV who are “successfully treated” (meaning that they no longer have ocular motor evidence for the presence of BPPV) continue to feel disequilibrium for some time (Özgirgin et al. 2024). Some literature refers to this as “residual dizziness following successful treatment of BPPV.”
There are several plausible mechanisms for “residual dizziness” (RD) following “successful treatment of BPPV.”
- Some literature describes persistent otoliths in the semicircular canals (Dispenza et al. 2019). This explanation suggests that although an examiner can no longer see ocular motor evidence of BPPV, there are residual otoliths in the semicircular canals which are sufficient to provoke symptoms, but insufficient to provoke corresponding ocular motor findings.
- Some literature suggests that otolith organ dysfunction accounts for RD. Although the mechanism of BPPV is that otoliths become dislodged from the gelatinous membranes in the otolith organs and enter the semicircular canals, this explanation for RD points to the fact that the otolith organs may not function correctly without sufficient otoliths in their proper place (Ismail et al. 2024). In support of this idea are published observations of abnormal vestibular evoked myogenic potentials in some patients with BPPV (Hong et al. 2008; Hoseinabadi et al. 2016; Korres et al. 2011; Lee et al. 2013; Oya et al. 2019; Scarpa et al. 2019; Singh and Apeksha 2016; Xu et al. 2016; Yang et al. 2008; Yetiser et al. 2014).
- Since afferent signals from the otolith organs feed in to autonomic function (Kim et al. 2022; Yamamoto et al. 2000), and since autonomic dysfunction can be associated with vertiginous sensations (Nakagawa et al. 1993; Pappas 2003), it is possible that in patients with BPPV (whose otolith organs are dysfunctional secondary to the loss of the otoliths) also have some degree of autonomic dysfunction (Kim and Lee 2014) that accounts for RD despite adequate treatment of BPPV.
- Some literature regarding fMRI in patients with BPPV identify functional changes (Chen et al. 2024a; Chen et al. 2024b; Fu et al. 2022; Lin et al. 2023). The mechanism of this is poorly understood, but suggests that in some patients, the presence of BPPV induces neuroplastic changes that may persist beyond the presence of BPPV — in other words, a maladaptive response.
- Another possibility is that BPPV triggers persistent postural perceptual dizziness (PPPD) (Casani et al. 2023; Habs et al. 2020).
The main risk factor for RD appears to be older age (Fu et al. 2023; Martellucci et al. 2016; Teggi et al. 2011). Other risk factors include longer duration of BPPV (Teggi et al. 2011; Teggi et al. 2013) and hypovitaminosis D (Wu et al. 2022).
The prognosis of RD is unclear. Some literature describes it as a “self-limiting” disorder (Martellucci et al. 2016) that tends to resolve “in 3 months without specific treatment” (Seok et al. 2008).
For patients who elect to attempt treatment for RD, the management is unclear. Continued vestibular rehabilitation therapy, such as with Cawthorne-Cooksey exercises or Brandt-Daroff maneuvers, may be helpful (Ersin and Serbetcioglu 2025), perhaps serving as a type of habituation. Betahistine has been suggested, but results are mixed, with some studies suggesting efficacy (Jalali et al. 2020) and others not (Acar et al. 2015). Some studies suggest that cognitive behavioral therapy (CBT) may play some role (Wan et al. 2018). Even in a patient who appears to have RD, it is medically reasonable to reassess periodically to monitor for whether there is true recurrence of BPPV.
§6: Prognosis of BPPV. Recurrence.
The natural history of BPPV is one of recurrence. One study (Luryi et al. 2018a) of 1105 patients found that after a first episode of BPPV had resolved, recurrence happened anywhere from 3 to 2496 days later; 56% of patients experienced recurrence within the first year, and 76% of patients experienced recurrence within 2 years. A patient’s vulnerability to recurrence (and its unpredictability) can provoke feelings of (if not formally diagnosable) anxiety and depression (Lee and Hur 2026).
Recurrences usually (but not always) involve the same semicircular canal that was most recently affected. Therefore, if a given vestibular treatment exercise clearly helps a bout of BPPV, but a patient then experiences what feels like a recurrence, it is medically quite reasonable to resume exactly the same exercise that was most recently helpful, because statistically it is likely to be correct. If resuming the previously successful exercise does, in fact, help, then no further intervention is needed. In contrast, if a recurrence fails to respond to a previously successful exercise, then a patient should have her eye movements examined again in order to determine whether the BPPV is “in the same place,” or whether the problem is actually still BPPV.
As discussed earlier (see the section above entitled, “Can recurrences of BPPV be prevented?”), there is emerging evidence that supplementation with vitamin D (and perhaps calcium) may reduce the rate of recurrence of BPPV in patients who have vitamin D deficiency; in contrast, in patients whose vitamin D levels are already normal, giving extra vitamin D does not appear to have any influence on the rate of recurrence of BPPV.
There is a modest literature suggesting that BPPV following head trauma is more likely to recur (Dlugaiczyk et al. 2011), though not all investigators share this viewpoint.
References
Acar B, Karasen RM, Buran Y (2015) Efficacy of medical therapy in the prevention of residual dizziness after successful repositioning maneuvers for Benign Paroxysmal Positional Vertigo (BPPV). B-ENT 11: 117-21
Achard S, Campion M, Parodi M, MacAskill M, Hochet B, Simon F, Rouillon I, Jonard L, Serey-Gaut M, Denoyelle F, Loundon N, Marlin S (2023a) Recurrent Benign Paroxysmal Positional Vertigo in DFNB16 Patients with Biallelic STRC Gene Deletions. Otol Neurotol 44: e241-e245. doi: 10.1097/MAO.0000000000003825
Achard S, Simon F, Denoyelle F, Marlin S (2023b) Recurrent benign paroxysmal positional vertigo in two DFNB16 siblings: A CARE case report. Eur Ann Otorhinolaryngol Head Neck Dis 140: 127-129. doi: 10.1016/j.anorl.2022.12.002
Akcay H, Ulu M, Kelebek S, Aladag I (2016) Benign Paroxysmal Positional Vertigo Following Sinus Floor Elevation in Patient with Antecedents of Vertigo. J Maxillofac Oral Surg 15: 351-4. doi: 10.1007/s12663-016-0891-9
Anagnostou E, Stamboulis E, Kararizou E (2014) Canal conversion after repositioning procedures: comparison of Semont and Epley maneuver. J Neurol 261: 866-9. doi: 10.1007/s00415-014-7290-2
Aron M, Lea J, Nakku D, Westerberg BD (2015) Symptom Resolution Rates of Posttraumatic versus Nontraumatic Benign Paroxysmal Positional Vertigo: A Systematic Review. Otolaryngol Head Neck Surg 153: 721-30. doi: 10.1177/0194599815594384
Babac S, Djeric D, Petrovic-Lazic M, Arsovic N, Mikic A (2014) Why do treatment failure and recurrences of benign paroxysmal positional vertigo occur? Otol Neurotol 35: 1105-10. doi: 10.1097/MAO.0000000000000417
Babic BB, Jesic SD, Milovanovic JD, Arsovic NA (2014) Unintentional conversion of benign paroxysmal positional vertigo caused by repositioning procedures for canalithiasis: transitional BPPV. Eur Arch Otorhinolaryngol 271: 967-73. doi: 10.1007/s00405-013-2494-0
Balatsouras DG, Koukoutsis G, Aspris A, Fassolis A, Moukos A, Economou NC, Katotomichelakis M (2017) Benign Paroxysmal Positional Vertigo Secondary to Mild Head Trauma. Ann Otol Rhinol Laryngol 126: 54-60. doi: 10.1177/0003489416674961
Balatsouras DG, Koukoutsis G, Ganelis P, Economou NC, Moukos A, Aspris A, Katotomichelakis M (2014) Benign paroxysmal positional vertigo secondary to vestibular neuritis. Eur Arch Otorhinolaryngol 271: 919-24. doi: 10.1007/s00405-013-2484-2
Baloh RW, Honrubia V, Jacobson K (1987) Benign positional vertigo: clinical and oculographic features in 240 cases. Neurology 37: 371-8. doi: 10.1212/wnl.37.3.371
Baloh RW, Solingen L, Sills AW, Honrubia V (1977) Caloric testing. 1. Effect of different conditions of ocular fixation. Ann Otol Rhinol Laryngol Suppl 86: 1-6.
Bárány E (1920) Diagnose von Krankheitserscheinungen im Bereiche des Otolithenapparates [Diagnosis of symptoms in the area of the otolith apparatus]. Acta Oto-Laryngologica 2: 434-437. doi: 10.3109/00016482009123103
Bennardo F, Barone S, Vocaturo C, Nucci L, Antonelli A, Giudice A (2022) Usefulness of Magnetic Mallet in Oral Surgery and Implantology: A Systematic Review. J Pers Med 12. doi: 10.3390/jpm12010108
Bhandari R, Bhandari A, Hsieh Y-H, Edlow J, Omron R (2023) Prevalence of Horizontal Canal Variant in 3,975 Patients With Benign Paroxysmal Positional Vertigo: A Cross-sectional Study. Neurology: Clinical Practice 13: e200191. doi: 10.1212/CPJ.0000000000200191
Bhattacharyya N, Gubbels SP, Schwartz SR, Edlow JA, El-Kashlan H, Fife T, Holmberg JM, Mahoney K, Hollingsworth DB, Roberts R, Seidman MD, Steiner RW, Do BT, Voelker CC, Waguespack RW, Corrigan MD (2017) Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update). Otolaryngol Head Neck Surg 156: S1-S47. doi: 10.1177/0194599816689667
Brauer HU (2009) Unusual complications associated with third molar surgery: a systematic review. Quintessence Int 40: 565-72.
Cakir BO, Ercan I, Cakir ZA, Turgut S (2006) Efficacy of postural restriction in treating benign paroxysmal positional vertigo. Arch Otolaryngol Head Neck Surg 132: 501-5. doi: 10.1001/archotol.132.5.501
Casani AP, Ducci N, Lazzerini F, Vernassa N, Bruschini L (2023) Preceding Benign Paroxysmal Positional Vertigo as a Trigger for Persistent Postural-Perceptual Dizziness: Which Clinical Predictors? Audiol Res 13: 942-951. doi: 10.3390/audiolres13060082
Casqueiro JC, Ayala A, Monedero G (2008) No more postural restrictions in posterior canal benign paroxysmal positional vertigo. Otol Neurotol 29: 706-9. doi: 10.1097/MAO.0b013e31817d01e8
Chambers BR, Gresty MA (1982) Effects of fixation and optokinetic stimulation on vestibulo-ocular reflex suppression. J Neurol Neurosurg Psychiatry 45: 998-1004.
Chang TP, Lin YW, Sung PY, Chuang HY, Chung HY, Liao WL (2016) Benign Paroxysmal Positional Vertigo after Dental Procedures: A Population-Based Case-Control Study. PLoS One 11: e0153092. doi: 10.1371/journal.pone.0153092
Chen J, Liu Z, Xie Y, Jin S (2023) Effects of vestibular rehabilitation training combined with anti-vertigo drugs on vertigo and balance function in patients with vestibular neuronitis: a systematic review and meta-analysis. Front Neurol 14: 1278307. doi: 10.3389/fneur.2023.1278307
Chen J, Zhao W, Yue X, Zhang P (2020) Risk Factors for the Occurrence of Benign Paroxysmal Positional Vertigo: A Systematic Review and Meta-Analysis. Front Neurol 11: 506. doi: 10.3389/fneur.2020.00506
Chen Z, Cai Y, Xiao L, Wei XE, Liu Y, Lin C, Liu D, Liu H, Rong L (2024a) Increased functional connectivity between default mode network and visual network potentially correlates with duration of residual dizziness in patients with benign paroxysmal positional vertigo. Front Neurol 15: 1363869. doi: 10.3389/fneur.2024.1363869
Chen Z, Liu Y, Lin C, Liu D, Xiao L, Liu H, Wei XE, Rong L (2024b) Altered parietal operculum cortex 2 functional connectivity in benign paroxysmal positional vertigo patients with residual dizziness: A resting-state fMRI study. CNS Neurosci Ther 30: e14570. doi: 10.1111/cns.14570
Chiarella G, Leopardi G, De Fazio L, Chiarella R, Cassandro E (2008) Benign paroxysmal positional vertigo after dental surgery. Eur Arch Otorhinolaryngol 265: 119-22. doi: 10.1007/s00405-007-0397-7
Choi JY, Park YM, Lee SH, Choi J, Hyun SW, Song JM, Kim HJ, Oh HJ, Kim JS (2021) Linear Vertigo in Benign Paroxysmal Positional Vertigo: Prevalence and Mechanism. Cerebellum 20: 160-168. doi: 10.1007/s12311-020-01196-6
Chua Wei De K, Gans R, Spinks S (2020) Demographic and clinical characteristics of 1599 BPPV patients. Journal of Otolaryngology-ENT Research 12: 1-11. doi: 10.15406/joentr.2020.12.00451
Crespi R, Cappare P, Gherlone E (2012) Sinus floor elevation by osteotome: hand mallet versus electric mallet. A prospective clinical study. Int J Oral Maxillofac Implants 27: 1144-50.
Crespi R, Cappare P, Gherlone E (2013) Electrical mallet provides essential advantages in maxillary bone condensing. A prospective clinical study. Clin Implant Dent Relat Res 15: 874-82. doi: 10.1111/j.1708-8208.2011.00432.x
Crespi R, Cappare P, Gherlone E (2014) A comparison of manual and electrical mallet in maxillary bone condensing for immediately loaded implants: a randomized study. Clin Implant Dent Relat Res 16: 374-82. doi: 10.1111/j.1708-8208.2012.00485.x
Damsaz M, Eshghpour M, Grillo R, Jafarpour K, Mazhari K, Samieirad S (2024) Assessment of Benign Paroxysmal Positional Vertigo (BPPV) Incidence Following Closed Sinus Lift and Ridge Splitting Surgeries: A Cohort Study. J Maxillofac Oral Surg 23: 1-6. doi: 10.1007/s12663-023-02007-1
De Stefano A, Dispenza F, Citraro L, Petrucci AG, Di Giovanni P, Kulamarva G, Mathur N, Croce A (2011) Are postural restrictions necessary for management of posterior canal benign paroxysmal positional vertigo? Ann Otol Rhinol Laryngol 120: 460-4. doi: 10.1177/000348941112000707
Deng M, Liu C, Jiang W, Wang F, Zhou J, Wang D, Wang Y (2020) A novel genetic variant associated with benign paroxysmal positional vertigo within the LOXL1. Mol Genet Genomic Med 8: e1469. doi: 10.1002/mgg3.1469
Devaiah AK, Andreoli S (2010) Postmaneuver restrictions in benign paroxysmal positional vertigo: an individual patient data meta-analysis. Otolaryngol Head Neck Surg 142: 155-9. doi: 10.1016/j.otohns.2009.09.013
Dispenza F, A DES, Costantino C, Rando D, Giglione M, Stagno R, Bennici E (2015) Canal switch and re-entry phenomenon in benign paroxysmal positional vertigo: difference between immediate and delayed occurrence. Acta Otorhinolaryngol Ital 35: 116-20.
Dispenza F, Mazzucco W, Mazzola S, Martines F (2019) Observational study on risk factors determining residual dizziness after successful benign paroxysmal positional vertigo treatment: the role of subclinical BPPV. Acta Otorhinolaryngol Ital 39: 347-352. doi: 10.14639/0392-100X-2247
Dix MR, Hallpike CS (1952a) The pathology symptomatology and diagnosis of certain common disorders of the vestibular system. Proc R Soc Med 45: 341-54.
Dix MR, Hallpike CS (1952b) The pathology, symptomatology and diagnosis of certain common disorders of the vestibular system. Ann Otol Rhinol Laryngol 61: 987-1016. doi: 10.1177/000348945206100403
Dlugaiczyk J, Siebert S, Hecker DJ, Brase C, Schick B (2011) Involvement of the anterior semicircular canal in posttraumatic benign paroxysmal positioning vertigo. Otol Neurotol 32: 1285-90. doi: 10.1097/MAO.0b013e31822e94d9
Ersin K, Serbetcioglu MB (2025) Evaluation of effective methods in the treatment of residual dizziness after BPPV: a randomized comparative clinical study. Eur Arch Otorhinolaryngol. doi: 10.1007/s00405-025-09780-4
Fife TD (2012) Positional dizziness. Continuum (Minneap Minn) 18: 1060-85. doi: 10.1212/01.CON.0000418376.80099.24
Foster CA, Zaccaro K, Strong D (2012) Canal conversion and reentry: a risk of Dix-Hallpike during canalith repositioning procedures. Otol Neurotol 33: 199-203. doi: 10.1097/MAO.0b013e31823e274a
Frenzel HGW (1956) Pragmatische Systematik in der Hals-Nasen-Ohren-Heilkunde [Practical methods of a systematic study of otorhinolaryngology]. Münchener Medizinische Wochenschrift 98: 972-5.
Fresnel A-J (1822) Mémoire sur un nuveau système d’éclairage des phares. Imprimerie Royale Lu à L’académie Des Sciences, Paris
Fu W, Bai Y, He F, Wei D, Wang Y, Shi Y, An X, Han J, Wang X (2022) The Association Between Precuneus Function and Residual Dizziness in Patients With Benign Paroxysmal Positional Vertigo. Front Neurol 13: 828642. doi: 10.3389/fneur.2022.828642
Fu W, He F, Bai Y, Wang Y, Wei D, Shi Y, An X, Han J, Wang X (2023) Assessment of residual dizziness after successful canalith repositioning maneuvre in benign paroxysmal positional vertigo patients: a questionnaire-based study. Eur Arch Otorhinolaryngol 280: 137-141. doi: 10.1007/s00405-022-07474-9
Fyrmpas G, Rachovitsas D, Haidich AB, Constantinidis J, Triaridis S, Vital V, Tsalighopoulos M (2009) Are postural restrictions after an Epley maneuver unnecessary? First results of a controlled study and review of the literature. Auris Nasus Larynx 36: 637-43. doi: 10.1016/j.anl.2009.04.004
Gacek RR (1978) Posterior ampullary nerve transection for benign paroxysmal positional vertigo. Trans Pa Acad Ophthalmol Otolaryngol 31: 190-3.
Galli M, Petracca T, Minozzi F, Gallottini L (2004) Complications in implant surgery by Summer’s technique: benign paroxysmal positional vertigo (BPPV). Minerva Stomatol 53: 535-41.
Ganji MR, Shafii Z, Hakemi MS (2019) Vitamin D Supplementation and Risk of Hypercalciuria in Stone Formers. Iran J Kidney Dis 13: 27-31.
Gauthier GM, Vercher JL (1990) Visual vestibular interaction: vestibulo-ocular reflex suppression with head-fixed target fixation. Exp Brain Res 81: 150-60.
Giannini S, Signorini L, Bonanome L, Severino M, Corpaci F, Cielo A (2015) Benign paroxysmal positional vertigo (BPPV): it may occur after dental implantology. A mini topical review. Eur Rev Med Pharmacol Sci 19: 3543-7.
Gizzi MS, Harper HW (2003) Suppression of the human vestibulo-ocular reflex by visual fixation or forced convergence in the dark, with a model interpretation. Curr Eye Res 26: 281-90.
Gordon CR, Gadoth N (2004) Repeated vs single physical maneuver in benign paroxysmal positional vertigo. Acta Neurol Scand 110: 166-9. doi: 10.1111/j.1600-0404.2004.00296.x
Habs M, Strobl R, Grill E, Dieterich M, Becker-Bense S (2020) Primary or secondary chronic functional dizziness: does it make a difference? A DizzyReg study in 356 patients. J Neurol 267: 212-222. doi: 10.1007/s00415-020-10150-9
Hanley K, O’Dowd T (2002) Symptoms of vertigo in general practice: a prospective study of diagnosis. Br J Gen Pract 52: 809-12.
Hart CW (1967) Ocular fixation and the caloric test. Laryngoscope 77: 2103-13. doi: 10.1288/00005537-196712000-00003
Helminski JO (2012) Differential Diagnosis and Treatment of Anterior Canal Benign Paroxysmal Positional Vertigo. Vestibular SIG Newsletter Special edition: BPPV.
Helminski JO, Janssen I, Hain TC (2008) Daily exercise does not prevent recurrence of benign paroxysmal positional vertigo. Otol Neurotol 29: 976-81. doi: 10.1097/MAO.0b013e318184586d
Hirvonen TP, Juhola M, Aalto H (2012) Suppression of spontaneous nystagmus during different visual fixation conditions. Eur Arch Otorhinolaryngol 269: 1759-62. doi: 10.1007/s00405-011-1824-3
Hong SM, Park DC, Yeo SG, Cha CI (2008) Vestibular evoked myogenic potentials in patients with benign paroxysmal positional vertigo involving each semicircular canal. Am J Otolaryngol 29: 184-7. doi: 10.1016/j.amjoto.2007.07.004
Hoseinabadi R, Pourbakht A, Yazdani N, Kouhi A, Kamali M (2016) The effects of abnormality of cVEMP and oVEMP on rehabilitation outcomes in patients with idiopathic benign paroxysmal positional vertigo. Eur Arch Otorhinolaryngol 273: 643-8. doi: 10.1007/s00405-015-3612-y
Hsu YT, Rosen PS, Choksi K, Shih MC, Ninneman S, Lee CT (2022) Complications of sinus floor elevation procedure and management strategies: A systematic review. Clin Implant Dent Relat Res 24: 740-765. doi: 10.1111/cid.13086
Ishiyama A, Jacobson KM, Baloh RW (2000) Migraine and benign positional vertigo. Ann Otol Rhinol Laryngol 109: 377-80. doi: 10.1177/000348940010900407
Ismail NM, Kabil SE, Abdel-Hamid EF (2024) Otolithic functions in patients with residual dizziness after successful repositioning manoeuvres for unilateral posterior canal BPPV. J Int Med Res 52: 3000605241249095. doi: 10.1177/03000605241249095
Jackson LE, Morgan B, Fletcher JC, Jr., Krueger WW (2007) Anterior canal benign paroxysmal positional vertigo: an underappreciated entity. Otol Neurotol 28: 218-22. doi: 10.1097/01.mao.0000247825.90774.6b
Jalali MM, Gerami H, Saberi A, Razaghi S (2020) The Impact of Betahistine versus Dimenhydrinate in the Resolution of Residual Dizziness in Patients with Benign Paroxysmal Positional Vertigo: A Randomized Clinical Trial. Ann Otol Rhinol Laryngol 129: 434-440. doi: 10.1177/0003489419892285
Jeong SH, Choi SH, Kim JY, Koo JW, Kim HJ, Kim JS (2009) Osteopenia and osteoporosis in idiopathic benign positional vertigo. Neurology 72: 1069-76. doi: 10.1212/01.wnl.0000345016.33983.e0
Jeong SH, Kim JS, Kim HJ, Choi JY, Koo JW, Choi KD, Park JY, Lee SH, Choi SY, Oh SY, Yang TH, Park JH, Jung I, Ahn S, Kim S (2020a) Prevention of benign paroxysmal positional vertigo with vitamin D supplementation: A randomized trial. Neurology 95: e1117-e1125. doi: 10.1212/WNL.0000000000010343
Jeong SH, Lee SU, Kim JS (2020b) Prevention of recurrent benign paroxysmal positional vertigo with vitamin D supplementation: a meta-analysis. J Neurol. doi: 10.1007/s00415-020-09952-8
Kansu L, Aydin E, Gulsahi K (2015) Benign paroxysmal positional vertigo after nonotologic surgery: case series. J Maxillofac Oral Surg 14: 113-5. doi: 10.1007/s12663-012-0356-8
Kaplan DM, Attal U, Kraus M (2003) Bilateral benign paroxysmal positional vertigo following a tooth implantation. J Laryngol Otol 117: 312-3. doi: 10.1258/00222150360600959
Karababa E, Balaban AN, Sunar A, Satar B (2025) The effects of the affected semicircular canal and nystagmus characteristics on the sensation of vertigo in benign paroxysmal positional vertigo. Praxis of Otorhinolaryngology 13: 194-202. doi: 10.5606/kbbu.2025.74875
Karlsen EA, Goetzinger CP, Hassanein R (1980) Effects of six conditions of ocular fixation on caloric nystagmus. Arch Otolaryngol 106: 474-6.
Katsarkas A (1999) Benign paroxysmal positional vertigo (BPPV): idiopathic versus post-traumatic. Acta Otolaryngol 119: 745-9. doi: 10.1080/00016489950180360
Katsarkas A, Kirkham TH (1982) Failure of suppression of post-caloric nystagmus by fixation. J Otolaryngol 11: 57-9.
Kim HA, Lee H (2014) Autonomic dysfunction as a possible cause of residual dizziness after successful treatment in benign paroxysmal positional vertigo. Clin Neurophysiol 125: 608-14. doi: 10.1016/j.clinph.2013.08.008
Kim JG, Lee JH, Lee SU, Choi JY, Kim BJ, Kim JS (2022) Utricular dysfunction in patients with orthostatic hypotension. Clin Auton Res 32: 431-444. doi: 10.1007/s10286-022-00890-1
Kim SK, Hong SM, Park IS, Choi HG (2019) Association Between Migraine and Benign Paroxysmal Positional Vertigo Among Adults in South Korea. JAMA Otolaryngol Head Neck Surg 145: 307-312. doi: 10.1001/jamaoto.2018.4016
Kisilevsky V, Bailie NA, Dutt SN, Rutka JA (2009) Lessons learned from the surgical management of benign paroxysmal positional vertigo: the University Health Network experience with posterior semicircular canal occlusion surgery (1988-2006). J Otolaryngol Head Neck Surg 38: 212-21.
Kniep R (2015) Otoconia: Mimicking a calcite-based functional material of the human body. From basic research to medical aspects. Pure and Applied Chemistry 87: 719-736. doi: doi:10.1515/pac-2015-0201
Korres S, Gkoritsa E, Giannakakou-Razelou D, Yiotakis I, Riga M, Nikolpoulos TP (2011) Vestibular evoked myogenic potentials in patients with BPPV. Med Sci Monit 17: CR42-47. doi: 10.12659/msm.881328
Kutlubaev MA, Xu Y, Hornibrook J (2019) Benign paroxysmal positional vertigo in Meniere’s disease: systematic review and meta-analysis of frequency and clinical characteristics. J Neurol. doi: 10.1007/s00415-019-09502-x
Lee G, Lee SG, Park HS, Kim BJ, Choi SJ, Choi JW (2019) Clinical characteristics and associated factors of canal switch in benign paroxysmal positional vertigo. J Vestib Res 29: 253-260. doi: 10.3233/VES-190667
Lee JD, Park MK, Lee BD, Lee TK, Sung KB, Park JY (2013) Abnormality of cervical vestibular-evoked myogenic potentials and ocular vestibular-evoked myogenic potentials in patients with recurrent benign paroxysmal postitional vertigo. Acta Otolaryngol 133: 150-3. doi: 10.3109/00016489.2012.723823
Lee NH, Ban JH, Lee KC, Kim SM (2010) Benign paroxysmal positional vertigo secondary to inner ear disease. Otolaryngol Head Neck Surg 143: 413-7. doi: 10.1016/j.otohns.2010.06.905
Lee SJ, Hur Y (2026) Living With the Fear of Recurrence in Benign Paroxysmal Positional Vertigo. Health Expect 29: e70551. doi: 10.1111/hex.70551
Letavernier E, Daudon M (2018) Vitamin D, Hypercalciuria and Kidney Stones. Nutrients 10. doi: 10.3390/nu10030366
Levo H, Aalto H, Petteri Hirvonen T (2004) Nystagmus measured with video-oculography: methodological aspects and normative data. ORL J Otorhinolaryngol Relat Spec 66: 101-4. doi: 10.1159/000079327
Lin C, Liu D, Liu Y, Chen Z, Wei X, Liu H, Wang K, Liu T, Xiao L, Rong L (2023) Altered functional activity of the precuneus and superior temporal gyrus in patients with residual dizziness caused by benign paroxysmal positional vertigo. Front Neurosci 17: 1221579. doi: 10.3389/fnins.2023.1221579
Lin GC, Basura GJ, Wong HT, Heidenreich KD (2012) Canal switch after canalith repositioning procedure for benign paroxysmal positional vertigo. Laryngoscope 122: 2076-8. doi: 10.1002/lary.23315
Lopez-Escamez JA, Lopez-Nevot A, Gamiz MJ, Moreno PM, Bracero F, Castillo JL, Salinero J (2000) [Diagnosis of common causes of vertigo using a structured clinical history]. Acta Otorrinolaringol Esp 51: 25-30.
Luryi AL, LaRouere M, Babu S, Bojrab DI, Zappia J, Sargent EW, Schutt CA (2019) Traumatic versus Idiopathic Benign Positional Vertigo: Analysis of Disease, Treatment, and Outcome Characteristics. Otolaryngol Head Neck Surg 160: 131-136. doi: 10.1177/0194599818797892
Luryi AL, Lawrence J, Bojrab DI, LaRouere M, Babu S, Zappia J, Sargent EW, Chan E, Naumann I, Hong RS, Schutt CA (2018a) Recurrence in Benign Paroxysmal Positional Vertigo: A Large, Single-Institution Study. Otol Neurotol 39: 622-627. doi: 10.1097/MAO.0000000000001800
Luryi AL, Schutt CA, Bojrab DI, LaRouere M, Zappia J, Sargent EW, Babu S (2018b) Causes of Persistent Positional Vertigo Following Posterior Semicircular Canal Occlusion for Benign Paroxysmal Positional Vertigo. Otol Neurotol 39: e1078-e1083. doi: 10.1097/MAO.0000000000001990
Manzari L, Tramontano M (2023) Otolithic and canal functions assessment during the acute phase of benign paroxysmal positional vertigo. Eur Arch Otorhinolaryngol. doi: 10.1007/s00405-023-08312-2
Martellucci S, Pagliuca G, de Vincentiis M, Greco A, De Virgilio A, Nobili Benedetti FM, Gallipoli C, Rosato C, Clemenzi V, Gallo A (2016) Features of Residual Dizziness after Canalith Repositioning Procedures for Benign Paroxysmal Positional Vertigo. Otolaryngol Head Neck Surg 154: 693-701. doi: 10.1177/0194599815627624
McGinnis PQ, Nebbia M, Saez L, Rudolph K (2009) Retrospective comparison of outcomes for patients with benign paroxysmal positional vertigo based on length of postural restrictions. J Geriatr Phys Ther 32: 168-73. doi: 10.1519/00139143-200932040-00005
Messina AM, Marini E (2018) Benign Paroxysmal Positional Vertigo After Piezosurgical Removal of Osseointegrated Implants. J Craniofac Surg 29: e739-e740. doi: 10.1097/SCS.0000000000004649
Molina A, Sanz-Sanchez I, Sanz-Martin I, Ortiz-Vigon A, Sanz M (2022) Complications in sinus lifting procedures: Classification and management. Periodontol 2000 88: 103-115. doi: 10.1111/prd.12414
Molnar EM, Torok N (1974) The effect of ocular fixation on the caloric nystagmus. ORL J Otorhinolaryngol Relat Spec 36: 76-84.
Moon SJ, Bae SH, Kim HD, Kim JH, Cho YB (2005) The effect of postural restrictions in the treatment of benign paroxysmal positional vertigo. Eur Arch Otorhinolaryngol 262: 408-11. doi: 10.1007/s00405-004-0836-7
Mostafa BE, Youssef TA, Hamad AS (2013) The necessity of post-maneuver postural restriction in treating benign paroxysmal positional vertigo: a meta-analytic study. Eur Arch Otorhinolaryngol 270: 849-52. doi: 10.1007/s00405-012-2046-z
Nakagawa H, Ohashi N, Kanda K, Watanabe Y (1993) Autonomic nervous system disturbance as etiological background of vertigo and dizziness. Acta Otolaryngol Suppl 504: 130-3. doi: 10.3109/00016489309128138
Nedzelski JM, Barber HO, McIlmoyl L (1986) Diagnoses in a dizziness unit. J Otolaryngol 15: 101-4.
Neuhauser HK (2007) Epidemiology of vertigo. Curr Opin Neurol 20: 40-6. doi: 10.1097/WCO.0b013e328013f432
Nuti D, Nati C, Passali D (2000) Treatment of benign paroxysmal positional vertigo: no need for postmaneuver restrictions. Otolaryngol Head Neck Surg 122: 440-4. doi: 10.1067/mhn.2000.97986
Oya R, Imai T, Takenaka Y, Sato T, Oshima K, Ohta Y, Inohara H (2019) Clinical significance of cervical and ocular vestibular evoked myogenic potentials in benign paroxysmal positional vertigo: a meta-analysis. Eur Arch Otorhinolaryngol 276: 3257-3265. doi: 10.1007/s00405-019-05674-4
Özgirgin ON, Kingma H, Manzari L, Lacour M (2024) Residual dizziness after BPPV management: exploring pathophysiology and treatment beyond canalith repositioning maneuvers. Frontiers in Neurology 15. doi: 10.3389/fneur.2024.1382196
Papacharalampous GX, Vlastarakos PV, Kotsis GP, Davilis D, Manolopoulos L (2012) The Role of Postural Restrictions after BPPV Treatment: Real Effect on Successful Treatment and BPPV’s Recurrence Rates. Int J Otolaryngol 2012: 932847. doi: 10.1155/2012/932847
Pappas DG, Jr. (2003) Autonomic related vertigo. Laryngoscope 113: 1658-71. doi: 10.1097/00005537-200310000-00005
Park S, Kim BG, Kim SH, Chu H, Song MY, Kim M (2013) Canal conversion between anterior and posterior semicircular canal in benign paroxysmal positional vertigo. Otol Neurotol 34: 1725-8. doi: 10.1097/MAO.0b013e318294227a
Parnes LS, Agrawal SK, Atlas J (2003) Diagnosis and management of benign paroxysmal positional vertigo (BPPV). CMAJ 169: 681-93.
Parnes LS, McClure JA (1990) Posterior semicircular canal occlusion for intractable benign paroxysmal positional vertigo. Ann Otol Rhinol Laryngol 99: 330-4. doi: 10.1177/000348949009900502
Penarrocha-Diago M, Rambla-Ferrer J, Perez V, Perez-Garrigues H (2008) Benign paroxysmal vertigo secondary to placement of maxillary implants using the alveolar expansion technique with osteotomes: a study of 4 cases. Int J Oral Maxillofac Implants 23: 129-32.
Pisani V, Mazzone S, Di Mauro R, Giacomini PG, Di Girolamo S (2015) A survey of the nature of trauma of post-traumatic benign paroxysmal positional vertigo. Int J Audiol 54: 329-33. doi: 10.3109/14992027.2014.989454
Pjetursson BE, Lang NP (2014) Sinus floor elevation utilizing the transalveolar approach. Periodontol 2000 66: 59-71. doi: 10.1111/prd.12043
Reddy KS, Shivu ME, Billimaga A (2015) Benign paroxysmal positional vertigo during lateral window sinus lift procedure: a case report and review. Implant Dent 24: 106-9. doi: 10.1097/ID.0000000000000188
Roberts RA, Gans RE, DeBoodt JL, Lister JJ (2005) Treatment of benign paroxysmal positional vertigo: necessity of postmaneuver patient restrictions. J Am Acad Audiol 16: 357-66. doi: 10.3766/jaaa.16.6.4
Rodriguez Gutierrez C, Rodriguez Gomez E (2007) Positional vertigo afterwards maxillary dental implant surgery with bone regeneration. Med Oral Patol Oral Cir Bucal 12: E151-3.
Sammartino G, Mariniello M, Scaravilli MS (2011) Benign paroxysmal positional vertigo following closed sinus floor elevation procedure: mallet osteotomes vs. screwable osteotomes. A triple blind randomized controlled trial. Clin Oral Implants Res 22: 669-72. doi: 10.1111/j.1600-0501.2010.01998.x
Scarpa A, Gioacchini FM, Cassandro E, Tulli M, Ralli M, Re M, Cassandro C (2019) Clinical application of cVEMPs and oVEMPs in patients affected by Meniere’s disease, vestibular neuritis and benign paroxysmal positional vertigo: a systematic review. Acta Otorhinolaryngol Ital 39: 298-307. doi: 10.14639/0392-100X-2104
Seok JI, Lee HM, Yoo JH, Lee DK (2008) Residual dizziness after successful repositioning treatment in patients with benign paroxysmal positional vertigo. J Clin Neurol 4: 107-10. doi: 10.3988/jcn.2008.4.3.107
Shaia WT, Zappia JJ, Bojrab DI, LaRouere ML, Sargent EW, Diaz RC (2006) Success of posterior semicircular canal occlusion and application of the dizziness handicap inventory. Otolaryngol Head Neck Surg 134: 424-30. doi: 10.1016/j.otohns.2005.10.035
Simoceli L, Bittar RS, Greters ME (2005) Posture restrictions do not interfere in the results of canalith repositioning maneuver. Braz J Otorhinolaryngol 71: 55-9. doi: 10.1016/s1808-8694(15)31285-4
Singh NK, Apeksha K (2016) Efficacy of cervical and ocular vestibular-evoked myogenic potentials in evaluation of benign paroxysmal positional vertigo of posterior semicircular canal. Eur Arch Otorhinolaryngol 273: 2523-32. doi: 10.1007/s00405-015-3867-3
Sokolovski A (1966) The influence of mental activity and visual fixation upon caloric-induced nystagmus in normal subjects. Acta Otolaryngol 61: 209-20.
Stacchi C, Bernardello F, Spinato S, Mura R, Perelli M, Lombardi T, Troiano G, Canullo L (2022) Intraoperative complications and early implant failure after transcrestal sinus floor elevation with residual bone height </=5 mm: A retrospective multicenter study. Clin Oral Implants Res 33: 783-791. doi: 10.1111/clr.13959
Strupp M, Bhandari A, Brandt T, Halmagyi MG, Kim JS, Kingma H, von Brevern M, Whitney SL, Zhang B, Zuma EMF, Zee DS, Schubert MC (2026) Benign Paroxysmal Positional Vertigo: The Case for Renaming It Peripheral Paroxysmal Positional Vertigo. Neurology 106: e214861. doi: 10.1212/WNL.0000000000214861
Strupp M, Fischer C, Hanss L, Bayer O (2014) The takeaway Frenzel goggles: a Fresnel-based device. Neurology 83: 1241-5. doi: 10.1212/WNL.0000000000000838
Su GN, Tai PW, Su PT, Chien HH (2008) Protracted benign paroxysmal positional vertigo following osteotome sinus floor elevation: a case report. Int J Oral Maxillofac Implants 23: 955-9.
Teggi R, Giordano L, Bondi S, Fabiano B, Bussi M (2011) Residual dizziness after successful repositioning maneuvers for idiopathic benign paroxysmal positional vertigo in the elderly. Eur Arch Otorhinolaryngol 268: 507-11. doi: 10.1007/s00405-010-1422-9
Teggi R, Quaglieri S, Gatti O, Benazzo M, Bussi M (2013) Residual dizziness after successful repositioning maneuvers for idiopathic benign paroxysmal positional vertigo. ORL J Otorhinolaryngol Relat Spec 75: 74-81. doi: 10.1159/000350255
Tomaz A, Gananca MM, Gananca CF, Gananca FF, Caovilla HH, Harker L (2009) Benign paroxysmal positional vertigo: concomitant involvement of different semicircular canals. Ann Otol Rhinol Laryngol 118: 113-7. doi: 10.1177/000348940911800206
Vernamonte S, Mauro V, Vernamonte S, Messina AM (2011) An unusual complication of osteotome sinus floor elevation: benign paroxysmal positional vertigo. Int J Oral Maxillofac Surg 40: 216-8. doi: 10.1016/j.ijom.2010.07.010
von Brevern M, Bertholon P, Brandt T, Fife T, Imai T, Nuti D, Newman-Toker D (2015) Benign paroxysmal positional vertigo: Diagnostic criteria. J Vestib Res 25: 105-17. doi: 10.3233/VES-150553
von Brevern M, Bertholon P, Brandt T, Fife T, Imai T, Nuti D, Newman-Toker D (2017) Benign paroxysmal positional vertigo: Diagnostic criteria Consensus document of the Committee for the Classification of Vestibular Disorders of the Barany Society. Acta Otorrinolaringol Esp 68: 349-360. doi: 10.1016/j.otorri.2017.02.007
von Brevern M, Radtke A, Lezius F, Feldmann M, Ziese T, Lempert T, Neuhauser H (2007) Epidemiology of benign paroxysmal positional vertigo: a population based study. J Neurol Neurosurg Psychiatry 78: 710-5. doi: 10.1136/jnnp.2006.100420
Walther LE, Westhofen M (2007) Presbyvertigo-aging of otoconia and vestibular sensory cells. J Vestib Res 17: 89-92.
Wan TJ, Yu YC, Zhao XG, Tang P, Gong YS (2018) Efficacy of betahistine plus cognitive behavioral therapy on residual dizziness after successful canalith repositioning procedure for benign paroxysmal positional vertigo. Neuropsychiatr Dis Treat 14: 2965-2971. doi: 10.2147/NDT.S182809
Wanner L, Manegold-Brauer G, Brauer HU (2013) Review of unusual intraoperative and postoperative complications associated with endosseous implant placement. Quintessence Int 44: 773-81. doi: 10.3290/j.qi.a29936
Wu Y, Han K, Han W, Fan Z, Zhou M, Lu X, Liu X, Li L, Du L (2022) Low 25-Hydroxyvitamin D Levels Are Associated With Residual Dizziness After Successful Treatment of Benign Paroxysmal Positional Vertigo. Front Neurol 13: 915239. doi: 10.3389/fneur.2022.915239
Xu H, Liang FY, Chen L, Song XC, Tong MC, Thong JF, Zhang QQ, Sun Y (2016) Evaluation of the utricular and saccular function using oVEMPs and cVEMPs in BPPV patients. J Otolaryngol Head Neck Surg 45: 12. doi: 10.1186/s40463-016-0125-7
Xu Y, Zhang Y, Lopez IA, Hilbers J, Griswold AJ, Ishiyama A, Blanton S, Liu XZ, Lundberg YW (2021) Identification of a genetic variant underlying familial cases of recurrent benign paroxysmal positional vertigo. PLoS One 16: e0251386. doi: 10.1371/journal.pone.0251386
Yamamoto KI, Kawasaki Y, Izumi R, Kubo T (2000) Assessment of the otolith-autonomic response using spectral analysis of the R-R interval and blood pressure. Otolaryngol Head Neck Surg 123: 582-6. doi: 10.1067/mhn.2000.106401
Yang WS, Kim SH, Lee JD, Lee WS (2008) Clinical significance of vestibular evoked myogenic potentials in benign paroxysmal positional vertigo. Otol Neurotol 29: 1162-6. doi: 10.1097/MAO.0b013e31818a0881
Yetiser S, Ince D, Gul M (2014) An analysis of vestibular evoked myogenic potentials in patients with benign paroxysmal positional vertigo. Ann Otol Rhinol Laryngol 123: 686-95. doi: 10.1177/0003489414532778
![]()