By Marcello Cherchi, MD PhD
For patients
“White matter disease” (WMD) refers to a pattern of abnormalities seen on brain imaging. These abnormalities tend to occur with age, and in some cases may cause the symptom of disequilibrium. Distinguishing whether disequilibrium is due to WMD or to something else may require checking several tests of balance function. Treatment of the disequilibrium with vestibular rehabilitation therapy is medically reasonable.
For clinicians
Overview
In clinical parlance the phrase “white matter disease” (WMD) refers to the radiographic findings of non-enhancing areas of T2 hyperintensity (on MRI) or hypointensity/hyperlucency (on CT) usually in the cerebral periventricular and deep white matter. This corresponds to several different histopathological findings, and may be the result of different pathobiological mechanisms. The prevalence of WMD increases with age. In some cases, WMD seems to be associated with the symptom of disequilibrium, though the mechanism by which this occurs is unclear, and not all individuals with WMD experience disequilibrium. In a patient with WMD complaining of disequilibrium it is sensible to screen for other more common causes. WMD is associated with poorer recovery from benign paroxysmal positional vertigo and vestibular neuritis, though whether this relationship is synergistic or merely coincidental is uncertain.
Introduction
In day-to-day clinical practice the phrase “white matter disease” (WMD) usually alludes to radiographic findings, typically in the periventricular and deep white matter areas of the cerebrum, of T2 hyperintensity on MRI, or hypointensity/hyperlucency on CT.
There are various metrics for white matter disease (Gouw et al. 2008), such as the ARWMC (age-related white matter changes) scale (Wahlund et al. 2001), the Fazekas scale (Fazekas et al. 1987; Fazekas et al. 1993) and the Scheltens scale (Scheltens et al. 1993). There are also various metrics for progression of white matter disease, such as the Rotterdam scale (Prins et al. 2004) and the Schmidt scale (Schmidt et al. 1999). None of these metrics has been universally adopted.
Epidemiology
The prevalence of WMD increases with age (Zhuang et al. 2018).
Pathophysiological mechanism of disease
White matter disease goes by other names, such as “leukoaraiosis,” “chronic microvascular ischemic changes” or “ischemic demyelination.” These phrases may carry unintended implications for different readers. For example, since the phrase “chronic microvascular ischemic changes” contains the term “ischemia,” it may seem logical to view this as a pathology resulting from discrete strokes, but this does not appear to be the case (Fujishima et al. 2000). The phrase “ischemic demyelination” contains the term “demyelination,” which may imply an autoimmune process, yet this does not appear to be the case either (Li and Zhao 2020).
Even when WMD is radiographically well-delimited, it is unclear why this would impair equilibrium. Theoretical explanations of this usually cite disruption of multiple networks as the most plausible mechanism (Ibitoye et al. 2022; Kaski et al. 2019).
Clinical presentation
If other causes of disequilibrium have been excluded, and WMD appears (by exclusion) to be the only pathology implicated, then the symptom of disequilibrium generally is insidious in onset and gradually progressive.
Physical examination
There are no physical examination findings that are specific or sensitive for disequilibrium from WMD.
Ocular motor examination
There are no ocular motor findings that are specific or sensitive for disequilibrium from WMD.
Testing: vestibular
There are no otovestibular test results that are specific or sensitive for disequilibrium from WMD.
Imaging
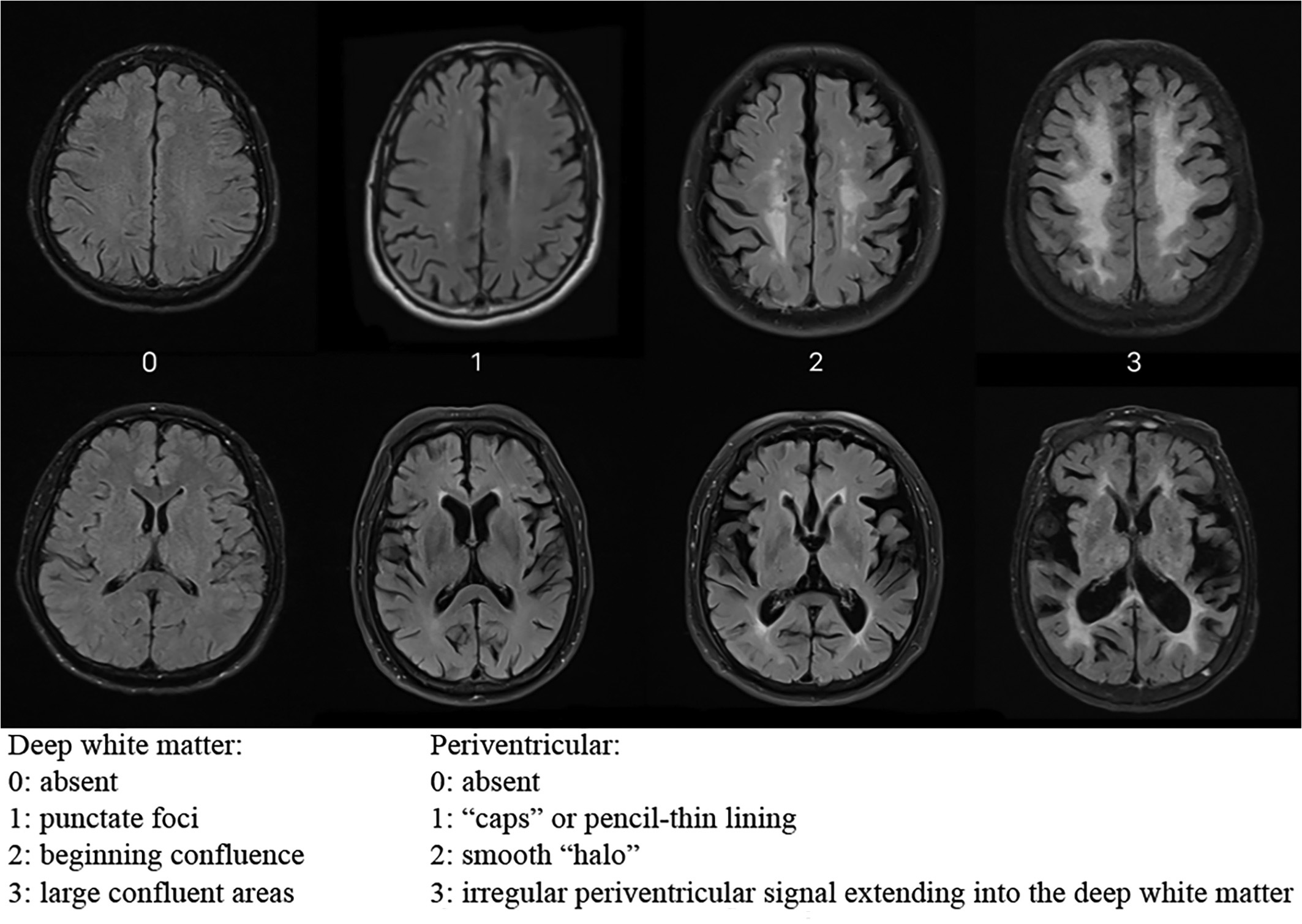
WMD typically involves the cerebral periventricular and deep white matter, and usually exhibits no contrast enhancement.
The Figure below, from Yu and colleagues (Yu et al. 2023), shows different degrees of WMD on brain MRI as rated on the Fazekas scale (Fazekas et al. 1987; Fazekas et al. 1993).
Histopathology
Autopsy studies report a variety of pathologies corresponding to the areas of radiographic abnormality, including microcystic infarcts, subependymal gliosis and others (Fazekas et al. 1993), suggesting that WMD is not a monolithic process.
Differential diagnosis: clinical
WMD may be the “final common pathway” of several age-associated microvascular pathologies, such as hypertension and dyslipidemia. But since the prevalence of WMD increases with age (Zhuang et al. 2018), the clinician must keep in mind that there are other causes of disequilibrium whose incidence also increases with advancing age.
It is well-established that the incidence of benign paroxysmal positional vertigo (BPPV) increases with age (von Brevern et al. 2007). There is modest evidence that patients with WMD are at a higher risk for developing BPPV (Yu et al. 2023). Interestingly, in patients with BPPV who also happen to have WMD, the symptom of disequilibrium tends to persist for longer than in patients without WMD (Zang et al. 2022). The nature of this relationship is unclear; for example, it is unknown whether the factors predisposing to WMD also predispose to BPPV, or whether the greater symptomatology is simply the synergistic effect of two diseases that happen to cause the symptom of disequilibrium through independent mechanisms.
Patients with WMD who happen to suffer a bout of vestibular neuritis (VN) may have greater difficulty recovering from VN. Again, the nature of this relationship is unclear; for example, it is unknown whether the factors underlying WMD impair the compensatory mechanisms that would otherwise promote a patient’s recovery, or whether mere co-occurrence of independent diseases has a synergistic effect.
It is well-known that patients with a history of migraine accumulate white matter hyperintensities at a greater rate than matched controls without migraine (Hamedani et al. 2013; Swartz and Kern 2004; Zhang et al. 2023). Some literature suggests that a clinical diagnosis of vestibular migraine increases the risk of WMD (Shen et al. 2023). However, this literature only documents associations; it does not establish causality.
Since WMD tends to occur in older individuals, in some instances it may be simply one contributor to the multifactorial disequilibrium resulting from age-related attrition of afferent and efferent functions required for properly functioning equilibrium.
Practically, if a patient with WMD is referred for a complaint of disequilibrium, it is sensible to screen for other more common causes of that symptom before concluding that WMD is the sole mechanism. A reasonable screening otovestibular workup may include cervical vestibular evoked myogenic potentials, ocular vestibular evoked myogenic potentials, video head impulse testing, videonystagmography and rotatory chair testing.
Differential diagnosis: radiographic
If white matter disease exhibits enhancement with radiographic contrast dye, then diseases such as autoimmune demyelinating processes and vasculitides should be considered.
If white matter disease also exhibits areas of hemorrhage of various ages, then cerebral amyloid angiopathy should be considered.
White matter disease occurring in specific distributions may suggest particular pathologies, such as CADASIL, CARASIL or Susac syndrome.
Treatment and prognosis
In a patient with WMD, management of vascular risk factors should be optimized. While this will not reverse the damage that is already present, it may retard the progression.
For the symptom of disequilibrium itself, vestibular rehabilitation therapy is always reasonable to consider, though controlled studies of this intervention are lacking.
References
Fazekas F, Chawluk JB, Alavi A, Hurtig HI, Zimmerman RA (1987) MR signal abnormalities at 1.5 T in Alzheimer’s dementia and normal aging. AJR Am J Roentgenol 149: 351-6. doi: 10.2214/ajr.149.2.351
Fazekas F, Kleinert R, Offenbacher H, Schmidt R, Kleinert G, Payer F, Radner H, Lechner H (1993) Pathologic correlates of incidental MRI white matter signal hyperintensities. Neurology 43: 1683-9. doi: 10.1212/wnl.43.9.1683
Fujishima M, Yao H, Terashi A, Tagawa K, Matsumoto M, Hara H, Akiguchi I, Suzuki K, Nishimaru K, Udaka F, Gyoten T, Takeuchi J, Hamada R, Yoshida Y, Ibayashi S (2000) Deep white matter lesions on MRI, and not silent brain infarcts are related to headache and dizziness of non-specific cause in non-stroke Japanese subjects. Intern Med 39: 727-31. doi: 10.2169/internalmedicine.39.727
Gouw AA, van der Flier WM, van Straaten EC, Pantoni L, Bastos-Leite AJ, Inzitari D, Erkinjuntti T, Wahlund LO, Ryberg C, Schmidt R, Fazekas F, Scheltens P, Barkhof F, group Ls (2008) Reliability and sensitivity of visual scales versus volumetry for evaluating white matter hyperintensity progression. Cerebrovasc Dis 25: 247-53. doi: 10.1159/000113863
Hamedani AG, Rose KM, Peterlin BL, Mosley TH, Coker LH, Jack CR, Knopman DS, Alonso A, Gottesman RF (2013) Migraine and white matter hyperintensities: the ARIC MRI study. Neurology 81: 1308-13. doi: 10.1212/WNL.0b013e3182a8235b
Ibitoye RT, Castro P, Cooke J, Allum J, Arshad Q, Murdin L, Wardlaw J, Kaski D, Sharp DJ, Bronstein AM (2022) A link between frontal white matter integrity and dizziness in cerebral small vessel disease. Neuroimage Clin 35: 103098. doi: 10.1016/j.nicl.2022.103098
Kaski D, Rust HM, Ibitoye R, Arshad Q, Allum JHJ, Bronstein AM (2019) Theoretical framework for “unexplained” dizziness in the elderly: The role of small vessel disease. Prog Brain Res 248: 225-240. doi: 10.1016/bs.pbr.2019.04.009
Li J, Zhao YM (2020) Clinical manifestations and imaging features of white matter demyelination in older patients. J Int Med Res 48: 300060520966806. doi: 10.1177/0300060520966806
Prins ND, van Straaten EC, van Dijk EJ, Simoni M, van Schijndel RA, Vrooman HA, Koudstaal PJ, Scheltens P, Breteler MM, Barkhof F (2004) Measuring progression of cerebral white matter lesions on MRI: visual rating and volumetrics. Neurology 62: 1533-9. doi: 10.1212/01.wnl.0000123264.40498.b6
Scheltens P, Barkhof F, Leys D, Pruvo JP, Nauta JJ, Vermersch P, Steinling M, Valk J (1993) A semiquantative rating scale for the assessment of signal hyperintensities on magnetic resonance imaging. J Neurol Sci 114: 7-12. doi: 10.1016/0022-510x(93)90041-v
Schmidt R, Fazekas F, Kapeller P, Schmidt H, Hartung HP (1999) MRI white matter hyperintensities: three-year follow-up of the Austrian Stroke Prevention Study. Neurology 53: 132-9. doi: 10.1212/wnl.53.1.132
Shen Y, Li D, Cao Q, Hu M, Hou Z, Xu L, Li Y, Hong D (2023) Risk factors of vestibular migraine-related brain white matter lesions. Acta Neurol Belg 123: 1833-1839. doi: 10.1007/s13760-022-02076-y
Swartz RH, Kern RZ (2004) Migraine is associated with magnetic resonance imaging white matter abnormalities: a meta-analysis. Arch Neurol 61: 1366-8.
von Brevern M, Radtke A, Lezius F, Feldmann M, Ziese T, Lempert T, Neuhauser H (2007) Epidemiology of benign paroxysmal positional vertigo: a population based study. J Neurol Neurosurg Psychiatry 78: 710-5. doi: 10.1136/jnnp.2006.100420
Wahlund LO, Barkhof F, Fazekas F, Bronge L, Augustin M, Sjogren M, Wallin A, Ader H, Leys D, Pantoni L, Pasquier F, Erkinjuntti T, Scheltens P, European Task Force on Age-Related White Matter C (2001) A new rating scale for age-related white matter changes applicable to MRI and CT. Stroke 32: 1318-22. doi: 10.1161/01.str.32.6.1318
Yu T, Zhang H, Yan YM, Liu YN, Huang XF, Qiao S, Yang Q, Li P, Jiang RC, Ma DC (2023) Correlation of idiopathic benign paroxysmal positional vertigo with cerebral small vessel disease. Am J Emerg Med 74: 140-145. doi: 10.1016/j.ajem.2023.09.048
Zang J, Jiang X, Feng S, Zhang H (2022) The influence of cerebral small vessel diseases on the efficacy of repositioning therapy and prognosis of benign paroxysmal positional vertigo. Int J Med Sci 19: 1227-1234. doi: 10.7150/ijms.73080
Zhang W, Cheng Z, Fu F, Zhan Z (2023) Prevalence and clinical characteristics of white matter hyperintensities in Migraine: A meta-analysis. Neuroimage Clin 37: 103312. doi: 10.1016/j.nicl.2023.103312
Zhuang FJ, Chen Y, He WB, Cai ZY (2018) Prevalence of white matter hyperintensities increases with age. Neural Regen Res 13: 2141-2146. doi: 10.4103/1673-5374.241465
![]()