By Marcello Cherchi, MD PhD
For patients
When a person suffers trauma to the ear, it sometimes results in a small middle ear bone (called the stapes) to enter part-way into the inner ear, which can cause hearing loss, tinnitus and disequilibrium. If after suffering ear trauma you are experiencing these symptoms, then you should consult with an otolaryngologist. Your doctor may consider checking a temporal bone CT. Many cases require surgical repair.
For clinicians
Overview
The native stapes footplate is normally attached via the annular ligament to the membrane of the oval window. In pathological states the native stapes can be partially detached (subluxation) or completely detached (luxation) from the oval window structures. A stapes prosthesis that was initially placed correctly can migrate (called “stapes migration”) and thereby protrude excessively into the vestibule. Luxation and subluxation of the stapes, or excessive protrusion of a stapedial prosthesis into the vestibule, can occur from trauma or as a complication of otologic surgery. Associated pathologies include perilymphatic fistula (PLF), pneumolabyrinth and (if traumatic) incudostapedial dislocation. Patients usually present with auditory and/or vestibular symptoms. Audiometry usually shows mixed hearing loss. The diagnosis can often be corroborated on high resolution temporal bone CT. Treatment is surgical.
Introduction
The native stapes footplate is normally attached via the annular ligament to the membrane of the oval window. In pathological states the native stapes can be partially detached (subluxation) or completely detached (luxation) from the oval window structures. A stapes prosthesis can protrude excessively into the vestibule. Luxation and subluxation of the stapes, or excessive protrusion of a stapedial prosthesis into the vestibule, can occur from trauma or as a complication of otologic surgery.
Epidemiology
The most common cause of (sub)luxation of a native stapes is penetrating trauma (Bogaerts et al. 2014; Chen et al. 2021; Hatano et al. 2009; Herman et al. 1996; Lee and Lee 2025; Neuenschwander et al. 2005). It has also been rarely reported after non-otologic trauma, such as after a whiplash injury (Trager et al. 2005).
Less commonly, (sub)luxation of the stapes has been reported as a complication of various otologic procedures (Lewis Jr 1961). For example, Ayache and colleagues (Ayache et al. 2006) report a native stapes luxation 2 years after cartilage tympanoplasty.
Otosclerosis is sometimes treated by placing a stapes prosthesis. This procedure is occasionally complicated by perilymphatic fistula (PLF) and/or excessive protrusion of the prosthesis into the vestibule (Toirkens and Kelders 2015). Ayache and colleagues report that such complications occur in 0.2% – 3% of cases (Ayache et al. 2007), resulting in “sensorineural hearing loss and/or vertigo postoperatively.” Even if a stapes prosthesis is initially placed correctly, it can subsequently move medially (“stapes migration”) and thereby protrude excessively into the vestibule.
Genetics
No genetic factors have been reported to confer greater vulnerability to native stapes (sub)luxation.
Pathophysiological mechanism of disease
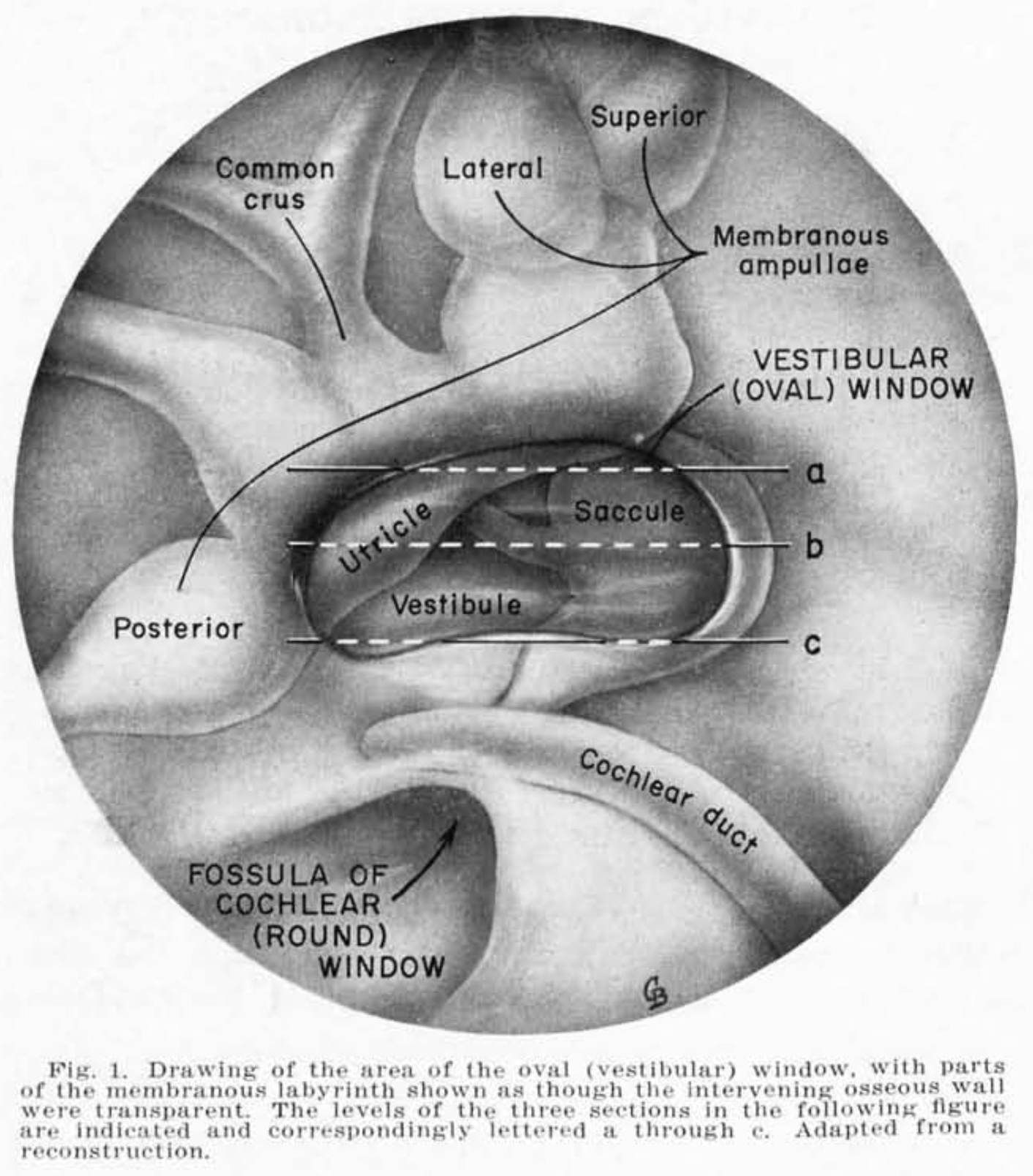
Immediately deep to the oval window is the vestibule. This tiny space is crowded with vestibularly-sensitive structures, as illustrated in the Figure below from Anson and colleagues (Anson et al. 1965).
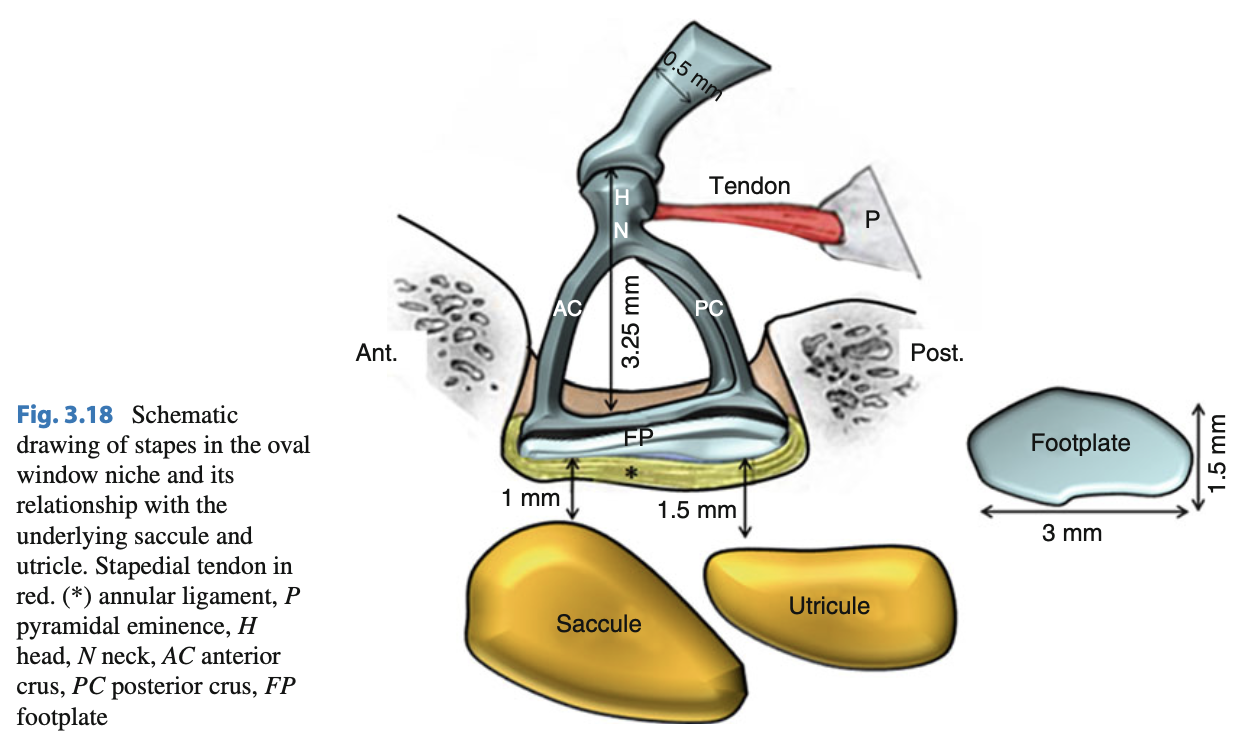
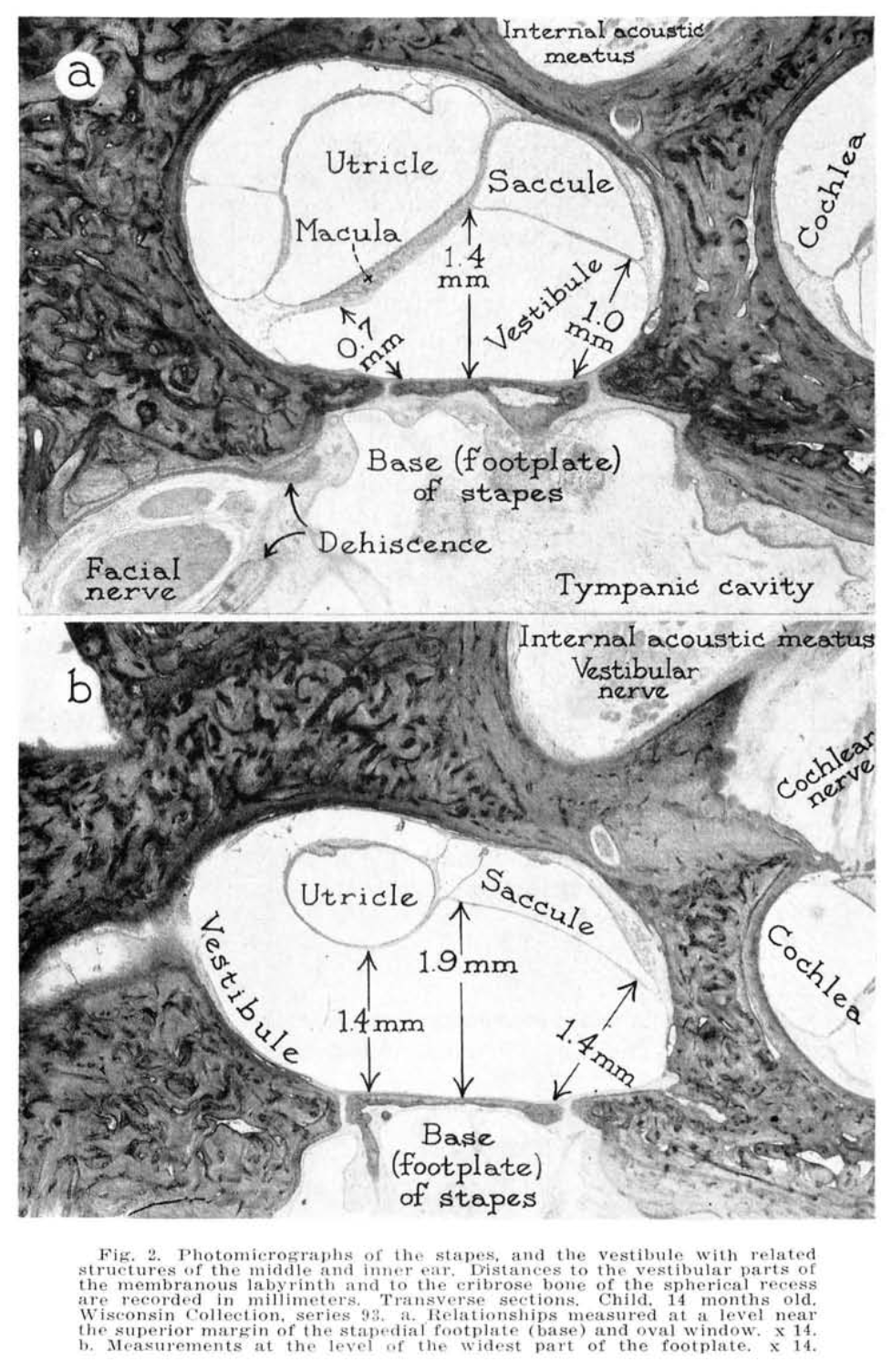
The healthy stapes is thus the otolith organs (saccule and utricle) (Backous et al. 1999). The relative disposition of the stapes and its neighboring structures is demonstrated in the Figure below from Mansour and colleagues (Mansour et al. 2013), and the Figure below showing a photomicrograph from Anson and colleagues (Anson et al. 1965).
Temporal bone studies suggest that the normative range of the relative position of the native stapes and the oval window varies within very narrow limits (Backous et al. 1999).
There is debate regarding the appropriate diameter (Huttenbrink 2003) and depth (Yehudai et al. 2010) of stapes prostheses.
Clinical presentation
Because stapedial (sub)luxation usually occurs after ear trauma, these patients typically present first to an otolaryngologist. It would be exceedingly unusual for such a patient to present initially to an otoneurologist.
Luxation and subluxation of a native stapes usually presents with some combination of audiologic symptoms (hearing loss, tinnitus) and vestibular symptoms (vertigo, ataxia) (Ayache et al. 2007; Ayache et al. 2006; Bogaerts et al. 2014; Lee and Lee 2025; Neuenschwander et al. 2005; Trager et al. 2005).
In those patients with a stapes prosthesis that becomes prolapsed or that migrates, symptoms can begin anywhere from immediately postsurgically to years later (Toirkens and Kelders 2015). We have evaluated a patient with a history of stapes prosthesis 13 years earlier who then developed vestibular symptoms two months after a bout of ipsilateral otitis media.
Physical examination
As far as physical examination is concerned, most publications on this topic focus descriptions on otologic penetrating trauma.
In the patients we have evaluated with radiographically confirmed stapes subluxation, physical examination has usually shown mixed hearing loss on the affected side, but physical examination and bedside infrared ocular motor testing has been normal.
Instrumented ocular motor examination
Very few articles describe nystagmus in these patients.
In patients with perilymphatic fistula (PLF), nystagmus induced by externally applied pressure or by Valsalva is weak and unreliable (Hain and Ostrowski 1997). It is reasonable to conjecture that this would also hold in circumstances where the PLF was the result of stapes subluxation/prolapse. In fact, Huttenbrink (Huttenbrink 2003) studied electronystagmography (ENG) in patients with a stapes prosthesis and reported that application of middle ear pressure by tympanometry could elicit nystagmus, even in asymptomatic individuals (in other words, patients with no complaints of vertigo).
Martins (Martins 1976) described two patients who suffered “traumatic dislocation of the stapes into the oval window” who exhibited a “change of the spontaneous nystagmus from an irritative to a paretic type,” suggesting that there was spontaneous horizontal nystagmus whose fast phase initially beat toward the affected side, then transitioned to beating away from the affected side.
Dieterich and colleagues (Dieterich et al. 1989) described the case of a musician (horn player) who developed left-sided stapes luxation (apparently without a discrete traumatic incident). Tullio’s phenomenon, induced by acoustic stimulation (480±20 Hz at 95 dB) in the affected (left) ear, elicited an ocular tilt reaction, which they described as, “dysconjugate concurrent upward movement of both eyes, ipsilateral hypertropia… counterclockwise ocular torsion, and head tilt (ipsilateral left ear up).”
Testing: auditory
The hearing loss in native stapes (sub)luxation can be sensorineural (Ayache et al. 2006; Bogaerts et al. 2014; Neuenschwander et al. 2005), conductive (Bogaerts et al. 2014; Lee and Lee 2025; Neuenschwander et al. 2005) or mixed (Chen et al. 2021).
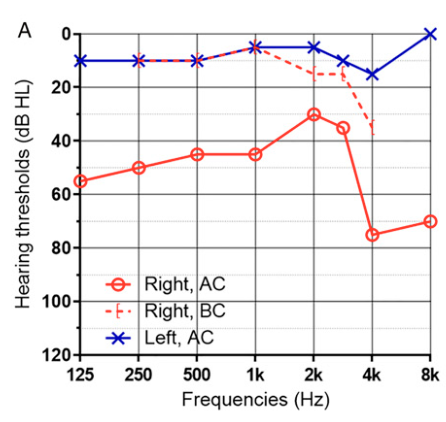
The Figure below, from Lee and colleagues (Lee and Lee 2025), shows an audiogram in a patient with right-sided stapes subluxation from penetrating trauma.
The hearing loss in a stapes prosthesis protrusion can be sensorineural or conductive (Swartz et al. 1986).
Testing: vestibular
As of this writing there were almost no published studies of vestibular testing specifically in patients with stapes subluxation (Huttenbrink 2003).
Vestibular tests requiring an acoustic stimulus (such as air-conducted vestibular evoked myogenic potentials, electrocochleography) would be non-diagnostic when the hearing loss is conductive or mixed.
Caloric testing may be relatively contraindicated in cases involving penetrating injuries.
It should be possible to study video head impulse testing (vHIT) in patients with stapes (sub)luxation, but as of this writing, there were no published studies on this.
Imaging
High resolution temporal bone CT is currently the imaging modality of choice for diagnosing (sub)luxation of the stapes (Ayache et al. 2006; Hatano et al. 2009; Herman et al. 1996; Lee and Lee 2025), or inappropriate protrusion of a stapes prosthesis (Ayache et al. 2007; Swartz et al. 1986; Toirkens and Kelders 2015).
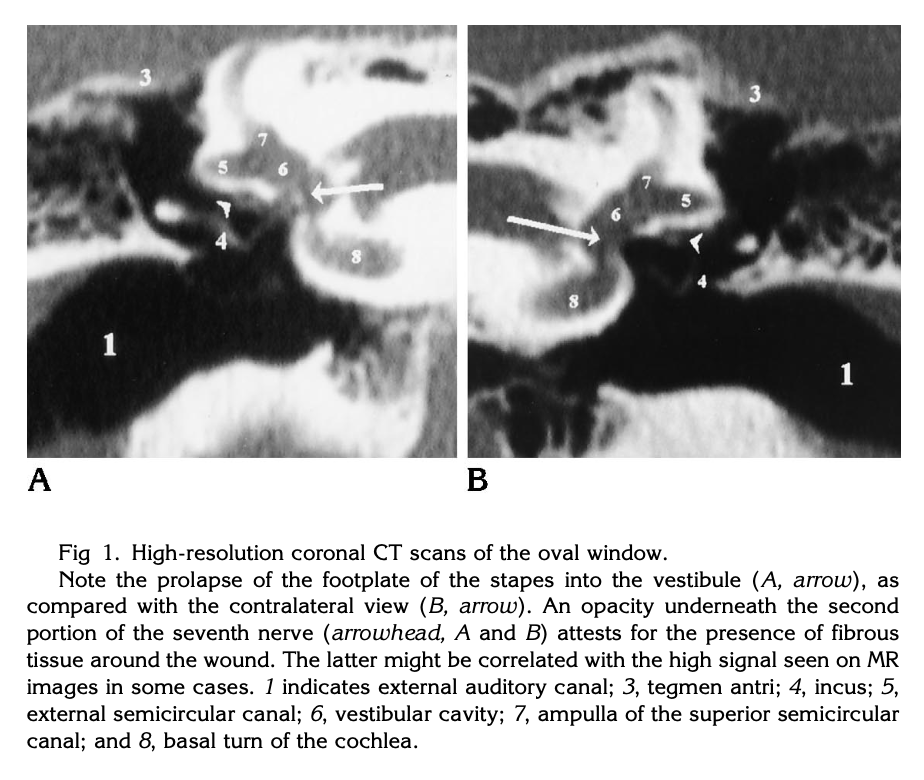
The Figure below, from Herman and colleagues (Herman et al. 1996), shows a temporal bone CT demonstrating luxation of the stapes into the vestibule following penetrating trauma.
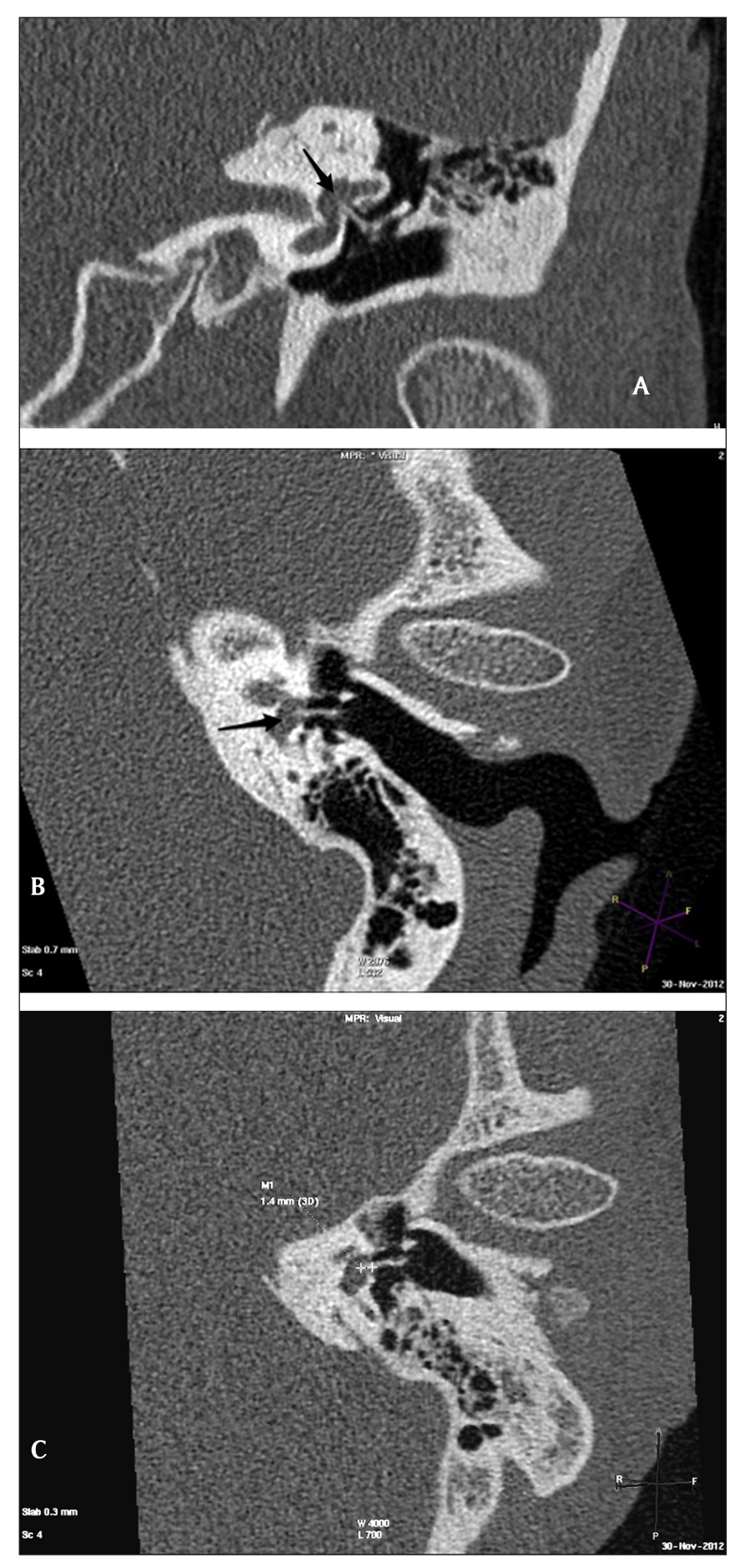
The Figure below, from Toirkens and colleagues (Toirkens and Kelders 2015), shows a temporal bone CT demonstrating protrusion of a stapes prosthesis into the vestibule.
Differential diagnosis
Stapes (sub)luxation is often accompanied by perilymphatic fistula (PLF) and pneumolabyrinth.
Management
Management of native stapes (sub)luxation (Bogaerts et al. 2014) and stapes prosthesis protrusion (Ayache et al. 2007) is surgical.
Prognosis
Bogaerts and colleagues (Bogaerts et al. 2014) reviewed literature on surgical outcomes and reported that, surgical repair has “variable hearing outcomes but offers complete resolution of vestibular symptoms in most cases.”
Hatano and colleagues (Hatano et al. 2009) report a case of stapes luxation in which after surgical repair, “the patient has been free from vertigo and has exhibited some recovery of his hearing.”
Lee and Lee (Lee and Lee 2025) report a case of stapes luxation in which, “Vertigo rapidly subsided after surgery, and hearing was improved to normal range. However, hearing loss at high frequencies was not recovered, probably because of inner ear damage due to the stapes depressed into the vestibule or surgical manipulation within the vestibule.”
Ayache and colleagues (Ayache et al. 2007) comment that prognosis is poor when stapes (sub)luxation evolves into labyrinthitis, or when granulomas develop.
References
Anson BJ, Donaldson JA, Warpeha RL, Winch TR (1965) Symposium: management of Meniere’s disease. II. Anatomic considerations. Laryngoscope 75: 1497-517. doi: 10.1002/lary.5540751002
Ayache D, Lejeune D, Williams MT (2007) Imaging of postoperative sensorineural complications of stapes surgery: a pictorial essay. Adv Otorhinolaryngol 65: 308-313. doi: 10.1159/000098850
Ayache D, Zaki Z, Wiener V, Williams MT (2006) Delayed luxation of the stapes into the vestibule after cartilage tympanoplasty. Otol Neurotol 27: 901-2. doi: 10.1097/01.mao.0000180481.26921.97
Backous DD, Minor LB, Aboujaoude ES, Nager GT (1999) Relationship of the utriculus and sacculus to the stapes footplate: anatomic implications for sound-and/or pressure-induced otolith activation. Ann Otol Rhinol Laryngol 108: 548-53. doi: 10.1177/000348949910800604
Bogaerts M, Waterval J, van Dinther J, Somers T, Zarowski A, Offeciers FE (2014) Treatment of traumatic stapediovestibular luxation: case report with the introduction of a new technique and review of literature. Otol Neurotol 35: 582-8. doi: 10.1097/MAO.0000000000000322
Chen B, Yang D, Xu Y, Zhou H (2021) [Traumatic incudostapedial joint dislocation with stapes footplate into the vestibular window and pneumolabyrinth: a case report]. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 35: 174-175. doi: 10.13201/j.issn.2096-7993.2021.02.019
Dieterich M, Brandt T, Fries W (1989) Otolith function in man. Results from a case of otolith Tullio phenomenon. Brain 112 ( Pt 5): 1377-92. doi: 10.1093/brain/112.5.1377
Hain TC, Ostrowski VB (1997) Limits of normal for pressure sensitivity in the fistula test. Audiol Neurootol 2: 384-390. doi: 10.1159/000259263
Hatano A, Rikitake M, Komori M, Irie T, Moriyama H (2009) Traumatic perilymphatic fistula with the luxation of the stapes into the vestibule. Auris Nasus Larynx 36: 474-8. doi: 10.1016/j.anl.2008.10.003
Herman P, Guichard JP, Van den Abbeele T, Tan CT, Bensimon JL, Marianowski R, Tran Ba Huy P (1996) Traumatic luxation of the stapes evidenced by high-resolution CT. AJNR Am J Neuroradiol 17: 1242-4.
Huttenbrink KB (2003) Biomechanics of stapesplasty: a review. Otol Neurotol 24: 548-57; discussion 557-9. doi: 10.1097/00129492-200307000-00004
Lee JM, Lee HJ (2025) Traumatic Stapes Luxation into the Vestibule. Ear Nose Throat J 104: 232-236. doi: 10.1177/01455613221106215
Lewis Jr ML (1961) Inner ear complications of stapes surgery. The Laryngoscope 71: 377-384. doi: https://doi.org/10.1288/00005537-196104000-00002
Mansour S, Magnan J, Haidar H, Nicolas K, Louryan S (2013) Middle Ear Contents. In: Mansour S, Magnan J, Haidar H, Nicolas K, Louryan S (eds) Comprehensive and Clinical Anatomy of the Middle Ear. Springer Berlin Heidelberg, Berlin, Heidelberg, pp 49-81
Martins M (1976) [Presentation and treatment of stapes dislocation and subluxation (author’s transl)]. HNO 24: 396-8.
Neuenschwander MC, Deutsch ES, Cornetta A, Willcox TO (2005) Penetrating middle ear trauma: a report of 2 cases. Ear Nose Throat J 84: 32-5.
Swartz JD, Lansman AK, Berger AS, Wolfson RJ, Bell G, Popky GL, Swartz NG (1986) Stapes prosthesis: evaluation with CT. Radiology 158: 179-82. doi: 10.1148/radiology.158.1.3940377
Toirkens JP, Kelders WPA (2015) Intravestibular Stapes Prosthesis Protrusion Causing Post Stapedectomy Vertigo. J Belg Soc Radiol 99: 92-94. doi: 10.5334/jbr-btr.951
Trager V, Seidl RO, Ernst A (2005) [Displacement of a stapes piston as a consequence of whiplash injury with head impact]. HNO 53: 163-5. doi: 10.1007/s00106-003-1031-7
Yehudai N, Masoud S, Most T, Luntz M (2010) Depth of stapes prosthesis in the vestibule: baseline values and correlation with stapedectomy outcome. Acta Otolaryngol 130: 904-8. doi: 10.3109/00016480903555424
![]()