By Marcello Cherchi, MD PhD
For patients
A perilymphatic fistula (PLF) is an abnormal hole connecting the inner ear and the middle ear. It often results from trauma. It presents with hearing symptoms (hearing loss, excessively sensitive sound, tinnitus) and disequilibrium. Symptoms are often worsened by pressure changes (e.g., sneezing, coughing) or by exposure to a burst of loud sound. The most confident way to diagnosis PLF is at surgery, during which the surgeon actually visualizes fluid coming out of the abnormal hole connecting the inner ear and middle ear. Other ways of testing for PLF have not been as successful. Treatment is surgery by an otolaryngologist. Surgery is not always successful, and even when surgery is initially successful, PLF can recur.
For clinicians
Overview
A perilymphatic fistula (PLF) is an abnormal connection between the inner ear and the middle ear via a hole in the oval window or round window or both. It is often caused by trauma of various sorts, and can occur at any age. It presents with aural, auditory and vestibular symptoms, often triggered or exacerbated by pressure changes (e.g., Valsalva, diving) or by loud noises. Visualization of the fistula at surgery is the best way to secure the diagnosis. Other testing modalities (imaging, otovestibular testing, assays on middle ear fluid) are inferior to surgical exploration. PLF should be differentiated from labyrinthitis, Ménière’s disease and semicircular canal dehiscence. Treatment of PLF is surgical repair, though it is not always successful. Even when surgical repair is initially successful, PLF can recur.
Introduction
Perilymphatic fistula (PLF) is a condition in which an abnormal communication (essentially, a hole) develops in either the oval window, or the round window, or both. This abnormal communication between the inner ear and the middle ear permits vestibular and cochlear hair cells to be stimulated abnormally, manifesting as various combinations of auditory and vestibular symptoms. There are numerous potential causes; it appears that the majority of cases occur following trauma. Diagnosis is difficult; surgical exploration (enabling the surgeon to visualize the middle ear) remains the best way to secure the diagnosis, but is obviously invasive. Limited studies suggest that imaging may play some role. Other tests (audiologic, otovestibular, blood tests) are controversial and not widely accepted. Some PLFs heal spontaneously; in other cases surgery may be curative, but is not always successful.
Epidemiology
Because it is difficult to diagnose PLF, the diagnosis is controversial. Consequently it has been difficult to arrive at useful statistics regarding its incidence and prevalence.
PLF can occur at any age; it can be congenital (Reilly 1989, Reilly and Kenna 1989, Weber, Perez et al. 1993, Weissman, Weber et al. 1994, deJong 1998); it can occur in the pediatric population (Healy, Friedman et al. 1978, Pappas, Simpson et al. 1988, Ruben and Yankelowitz 1989, Weber, Kelly et al. 1994, Kim, Kazahaya et al. 2001, Nakashima, Sone et al. 2003, Rawal, Zhao et al. 2021), in young adults (Fitzgerald 1996), in middle and older age.
Pathophysiology
An understanding of PLF requires some brief comments on anatomy, hydraulics and physiology.
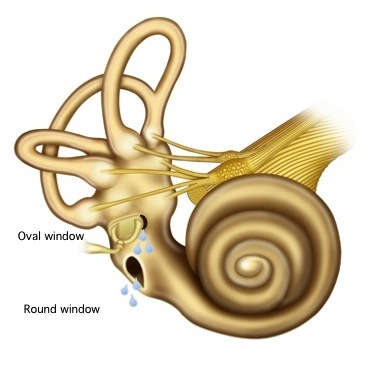
The interface between the inner ear and the middle ear consists of the oval window (to which the stapes footplate is attached) and the round window; both of these “windows” are covered by a soft membrane that can bulge inward or outward. Vibrations (typically from sound) cause an oscillating (inward and outward) piston-like motion of the stapes footplate. If the oval window were the only interface, then the stapes would barely be able to move the round window because inner ear fluid is effectively incompressible. However, the round window oscillates in a direction opposite that of the oval window; in other words, when the stapes pushes the oval window inwards, the round window bulges outwards, and vice versa. This arrangement makes it possible for vibration of the stapes footplate to be transduced into movement of the perilymph/endolymph and propagate through the labyrinth, usually stimulating hair cells in the cochlea which gets perceived as sound.
If the integrity of the oval window or round window is disrupted, then the overall resistance of the system (in a hydraulic sense) is reduced. There are several consequences to this reduced resistance.
- First, it will be easier to stimulate the inner ear with regular stimuli (such as sound). This can lead to perceiving sounds as louder in the affected ear.
- Second, the labyrinth may be stimulated by phenomena that would not normally do so. This can lead, for example, to auditory and vestibular symptoms triggered by Valsalva (such as during coughing, sneezing, etc.).
- Third, hair cells that are not normally stimulated by sound (specifically, vestibular hair cells) may get stimulated. This can lead to Tullio’s phenomenon.
PLF can involve the oval window, or the round window, or both, as illustrated in the Figure below.
Etiology
PLF has been reported in a broad variety of circumstances. The majority of cases reported occur in the context of some sort of trauma (Fee 1968, Lehrer, Poole et al. 1980, Glasscock, Hart et al. 1992, Fitzgerald 1995, Kim, Kazahaya et al. 2001, Gunesh and Huber 2003, Whitelaw and Young 2005, Nishiike, Hyo et al. 2008, Tsubota, Shojaku et al. 2009, Khoo and Tan 2011, Prisman, Ramsden et al. 2011, Fife and Giza 2013, Osetinsky, Hamilton et al. 2017, Kita, Kim et al. 2019, Rawal, Zhao et al. 2021, Koksal, Ayyildiz et al. 2022). A non-exhaustive list of potential etiologies is shown below.
Various sorts of trauma
- Barotrauma (Pullen 1992, Sheridan, Hetherington et al. 1999, McGhee and Dornhoffer 2000, Shupak 2006, Ahn, Son et al. 2019), particularly diving (Sheridan, Hetherington et al. 1999, Shupak 2006, Morvan, Gempp et al. 2016).
- In the context of the “common cold” (Klokker and Vesterhauge 2005), during which presumably a person is coughing and/or sneezing.
- Sneezing (Comacchio and Mion 2018).
- Nose blowing (Lee, Kwon et al. 2015).
- Vehicular airbag trauma (Ferber-Viart, Postec et al. 1998).
- Cotton swab use (Smith, Darrat et al. 2012).
- Stapes luxation (Hatano, Rikitake et al. 2009, Khoo and Tan 2011).
- Whiplash (Markou, Rachovitsas et al. 2014).
- Lightning strike (Sun, Simons et al. 2006, Kilic, Genc et al. 2017).
Pathologies that can potentially erode into the inner ear
- Cholesteatoma (Gormley 1986, Magliulo, Terranova et al. 1997).
- Granuloma (Kuhweide, van de Steene et al. 2007).
- Mastoiditis (McCabe 1984).
- Otitis media (Bluestone 1988).
Surgical complications
- Complication of stapes surgery (Albera, Canale et al. 2004).
- Complication of surgical drilling elsewhere in the temporal bone (Tsunoda, Anzai et al. 2021).
- Complication of transtympanic injection (Qureshi and Zeitler 2021).
- Migration of tympanostomy tube (Hajiioannou, Bathala et al. 2009).
There is a somewhat contentious discussion in the literature regarding whether PLF can also occur spontaneously (Pashley and Shapiro 1978, Ruben and Yankelowitz 1989, Gibson 1993, Meyerhoff 1993, Cole 1995, Kohut, Hinojosa et al. 1995, Kohut, Hinojosa et al. 1995, Collison and Pons 2004).
Clinical presentation
PLFs usually present with some combination of aural symptoms (e.g., fullness), auditory symptoms (hearing loss, hyperacusis, tinnitus) and vestibular symptoms (disequilibrium).
The symptoms often have episodic exacerbations, sometimes precipitated by pressure changes, whether internally generated (e.g., Valsalva while sneezing, coughing, blowing the nose, straining at stool) or externally generated (e.g., airplane ascent/descent, diving).
In some cases the symptoms are chronic, though in such cases the baseline symptoms are generally punctuated by acute exacerbations, as described earlier.
Diagnosis: physical examination
Often physical examination is normal. However, in some cases it may be possible to observe a bedside Tullio’s phenomenon by presenting a loud noise that elicits an ocular motor response (usually an oscillatory nystagmus). In other cases it may be possible to increase middle ear pressure (either with a pneumatic otoscope, or by applying pressure on the tragus) and observe nystagmus (Casale, Errante et al. 2014).
Diagnosis: imaging
Since PLF involves a very small hole in very small structures, it is difficult for this to be captured on contemporary imaging. Nevertheless, a number of studies and case series have collected radiographic observations (Nakashima, Sone et al. 2003, Ehmer, Booth et al. 2010, Venkatasamy, Al Ohraini et al. 2020), with some focusing on CT (Weissman, Weber et al. 1994, Kvestad, Kvaerner et al. 2001, Bozorg Grayeli, Bensimon et al. 2020) and others focusing on MRI (Morris, Kil et al. 1993, Algin, Bercin et al. 2012, Dubrulle, Chaton et al. 2020).
Diagnosis: audiologic and vestibular testing
A variety of otovestibular tests have been explored for the diagnosis of PLF, including:
- Audiometry (Fukaya and Nomura 1988) and “positional audiometry” (Hazell, Fraser et al. 1992).
- Electrocochleography (Arenberg, Ackley et al. 1988, Campbell and Parnes 1992, Campbell and Savage 1992, Campbell, Savage et al. 1992, Gibson 1992, Morris 1994, Sass, Densert et al. 1997) and “positional electrocochleography” (Campbell and Abbas 1993, Campbell and Abbas 1994).
- Otoacoustic emissions (Kokesh, Norton et al. 1994).
- Vestibular evoked myogenic potentials (Suzuki, Kitajima et al. 2003, Modugno, Magnani et al. 2006).
- Caloric testing (Dapsit, Churchill et al. 1980, Suzuki, Kitajima et al. 2003).
- Computerized dynamic posturography (Black, Lilly et al. 1990, Shepard, Telian et al. 1992, Selmani, Ishizaki et al. 2004, Pyykko, Selmani et al. 2012).
Ultimately, none of these methods has been widely accepted as diagnostic of PLF.
Diagnosis: laboratory tests on middle ear fluid
Although surgery remains considered the best way to diagnose PLF, sometimes the surgeon will not find clear evidence of PLF intraoperatively (Aso and Gibson 1994, Morris 1994, Haubner, Rohrmeier et al. 2012). On the possibilities that a fistula is very small, or has recently healed, some efforts have been directed at laboratory assays for fluid found in the middle ear at surgery with the goal of confirming/refuting the clinically suspected diagnosis of PLF. The main assays that have been studied are for beta-2-transferrin (Bassiouny, Hirsch et al. 1992, Skedros, Cass et al. 1993, Weber, Kelly et al. 1994, Weber, Bluestone et al. 1995, Delaroche, Bordure et al. 1996, Bluestone 1999), beta trace protein (Michel, Petereit et al. 2005, Bachmann-Harildstad, Stenklev et al. 2011) and cochlin-tomoprotein (Kataoka, Ikezono et al. 2013, Matsuda, Sakamoto et al. 2017, Fujita, Kobayashi et al. 2019, Lee, Ochi et al. 2020). None of these has been widely accepted.
Diagnosis: surgery
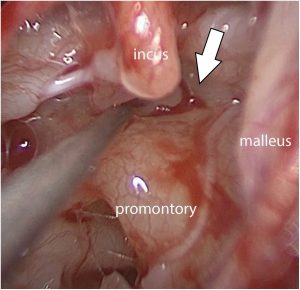
Surgery remains the gold standard for diagnosing PLF (Sekula and Wlodyka 1982, Yanagihara and Nishioka 1987, Poe, Rebeiz et al. 1992, Harvey and Millen 1994, Ogawa, Kanzaki et al. 1994, Poe and Bottrill 1994, Selmani, Pyykko et al. 2002, Alzahrani, Fadous et al. 2015, Prenzler, Schwab et al. 2018, Heilen, Lang et al. 2020). In this case, “surgery” means accessing the middle ear space either by myringotomy or by endoscopy, and observing the oval and round windows to detect whether fluid is seeping from them. While this remains the gold standard, it is imperfect, in that (1) it is invasive; and (2) many cases of clinically suspected PLF show no evidence of it during surgery (Aso and Gibson 1994, Morris 1994, Haubner, Rohrmeier et al. 2012).
The Figure below is a photograph of an endoscopic procedure visualizing perilymphatic leak from the anterior oval window from Rawal and colleagues (Rawal, Zhao et al. 2021).
Diagnosis: differential diagnosis
A number of diseases besides PLF can cause auditory and vestibular symptoms. While the differential diagnosis can be broad, the main considerations include:
- Chronic symptoms from PLF can be difficult to differentiate from labyrinthitis.
- Episodic symptoms from PLF can be difficult to differentiate from Ménière’s disease (Arenberg, May et al. 1974, Fitzgerald 2001).
- Chronic and episodic symptoms from PLF can be difficult to differentiate from semicircular canal dehiscence (Weinreich and Carey 2019).
- PLF can co-exist with other otologic pathologies, such as lateral semicircular canal dehiscence (Yaniv, Hacking et al. 1986, Yaniv and Hacking 1987).
Treatment
Surgical repair of PLF remains the mainstay of treatment (Lehrer, Rubin et al. 1984, Palva and Ramsay 1989, House, Morris et al. 1991, Black, Pesznecker et al. 1992, Deguine, Latil d’Albertas et al. 1995, Fitzgerald, Getson et al. 1997, Weider 1997, Maitland 2001, Weber, Bluestone et al. 2003, Kimitsuki, Hara et al. 2004, Omichi, Kariya et al. 2018, Ahn, Son et al. 2019, Rawal, Zhao et al. 2021). However, it must be kept in mind that surgery is not always successful (Heilen, Lang et al. 2020), and even if surgery is initially successful, PLF can recur (Gyo, Kobayashi et al. 1994).
Given that surgery is invasive and not always successful, a number of other treatments have been investigated, including autologous blood patch(Garg and Djalilian 2009, Foster 2016) and ventriculoperitoneal shunt (Weider, Roberts et al. 2005, Lollis, Weider et al. 2006). However, none of these has had the same rate of success as surgery.
Prognosis
Prognosis of PLF, both treated and untreated, is quite variable (Kubo, Kohno et al. 1993, Weber, Bluestone et al. 2003, Tsubota, Shojaku et al. 2009), and often these patients have long-term follow-up with an otolaryngologist.
References
Ahn J, Son SE, Choi JE, Cho YS, Chung WH (2019) Surgical Outcomes on Hearing and Vestibular Symptoms in Barotraumatic Perilymphatic Fistula. Otol Neurotol 40: e356-e363. doi: 10.1097/MAO.0000000000002160
Albera R, Canale A, Lacilla M, Cavalot AL, Ferrero V (2004) Delayed vertigo after stapes surgery. Laryngoscope 114: 860-2. doi: 10.1097/00005537-200405000-00013
Algin O, Bercin S, Akgunduz G, Turkbey B, Cetin H (2012) Evaluation of labyrinthine fistula by MR cisternography. Emerg Radiol 19: 557-60. doi: 10.1007/s10140-012-1050-3
Alzahrani M, Fadous R, Dufour JJ, Saliba I (2015) Perilymphatic fistulas: can we predict the diagnosis? Eur Arch Otorhinolaryngol 272: 1885-91. doi: 10.1007/s00405-014-3007-5
Arenberg IK, Ackley RS, Ferraro J, Muchnik C (1988) ECoG results in perilymphatic fistula: clinical and experimental studies. Otolaryngol Head Neck Surg 99: 435-43. doi: 10.1177/019459988809900501
Arenberg IK, May M, Stroud MH (1974) Perilymphatic fistula: an unusual cause of of Meniere’s syndrome in a prepubertal child. Laryngoscope 84: 243-6. doi: 10.1288/00005537-197402000-00005
Aso S, Gibson WP (1994) Perilymphatic fistula with no visible leak of fluid into the middle ear: a new method of intraoperative diagnosis using electrocochleography. Am J Otol 15: 96-100.
Bachmann-Harildstad G, Stenklev NC, Myrvoll E, Jablonski G, Klingenberg O (2011) beta-trace protein as a diagnostic marker for perilymphatic fluid fistula: a prospective controlled pilot study to test a sample collection technique. Otol Neurotol 32: 7-10. doi: 10.1097/mao.0b013e3181fc74d0
Bassiouny M, Hirsch BE, Kelly RH, Kamerer DB, Cass SP (1992) Beta 2 transferrin application in otology. Am J Otol 13: 552-5.
Black FO, Lilly DJ, Peterka RJ, Shupert C, Hemenway WG, Pesznecker SC (1990) The dynamic posturographic pressure test for the presumptive diagnosis of perilymph fistulas. Neurol Clin 8: 361-74.
Black FO, Pesznecker S, Norton T, Fowler L, Lilly DJ, Shupert C, Hemenway WG, Peterka RJ, Jacobson ES (1992) Surgical management of perilymphatic fistulas: a Portland experience. Am J Otol 13: 254-62.
Bluestone CD (1988) Otitis media and congenital perilymphatic fistula as a cause of sensorineural hearing loss in children. Pediatr Infect Dis J 7: S141-5. doi: 10.1097/00006454-198811001-00004
Bluestone CD (1999) Implications of beta-2 transferrin assay as a marker for perilymphatic versus cerebrospinal fluid labyrinthine fistula. Am J Otol 20: 701.
Bozorg Grayeli A, Bensimon JL, Guyon M, Aho-Glele S, Toupet M (2020) Detection of perilymphatic fistula in labyrinthine windows by virtual endoscopy and variation of reconstruction thresholds on CT scan. Acta Otolaryngol 140: 270-276. doi: 10.1080/00016489.2020.1715472
Campbell KC, Abbas PJ (1993) Electrocochleography with postural changes in perilymphatic fistula and Meniere’s disease: case reports. J Am Acad Audiol 4: 376-83.
Campbell KC, Abbas PJ (1994) Electrocochleography with postural changes in perilymphatic fistula. Animal studies. Ann Otol Rhinol Laryngol 103: 474-82. doi: 10.1177/000348949410300609
Campbell KC, Parnes L (1992) Electrocochleographic recordings in chronic and healed perilymphatic fistula. J Otolaryngol 21: 213-7.
Campbell KC, Savage MM (1992) Electrocochleographic recordings in acute and healed perilymphatic fistula. Arch Otolaryngol Head Neck Surg 118: 301-4. doi: 10.1001/archotol.1992.01880030089018
Campbell KC, Savage MM, Harker LA (1992) Electrocochleography in the presence and absence of perilymphatic fistula. Ann Otol Rhinol Laryngol 101: 403-7. doi: 10.1177/000348949210100505
Casale M, Errante Y, Sabatino L, Incammisa A, Salvinelli F, Quattrocchi CC (2014) Perilimphatic fistula test: a video clip demonstration. Eur Rev Med Pharmacol Sci 18: 3549-50.
Cole GG (1995) Validity of spontaneous perilymphatic fistula. Am J Otol 16: 815-9.
Collison PJ, Pons KC (2004) “Spontaneous” perilymph fistula: a case report. Ann Otol Rhinol Laryngol 113: 329-34. doi: 10.1177/000348940411300413
Comacchio F, Mion M (2018) Sneezing and Perilymphatic Fistula of the Round Window: Case Report and Systematic Review of the Literature. J Int Adv Otol 14: 106-111. doi: 10.5152/iao.2018.4336
Dapsit CP, Churchill D, Linthicum FH, Jr. (1980) Diagnosis of perilymph fistula using ENG and impedance. Laryngoscope 90: 217-223. doi: PMID: 7354689
Deguine O, Latil d’Albertas D, Fraysse B (1995) Comparison of postoperative results in suspected and confirmed cases of perilymphatic fistula. Rev Laryngol Otol Rhinol (Bord) 116: 95-8.
deJong AL (1998) Congenital perilymphatic fistula. Arch Otolaryngol Head Neck Surg 124: 1279-81. doi: 10.1001/archotol.124.11.1279
Delaroche O, Bordure P, Lippert E, Sagniez M (1996) Perilymph detection by beta 2-transferrin immunoblotting assay. Application to the diagnosis of perilymphatic fistulae. Clin Chim Acta 245: 93-104. doi: 10.1016/0009-8981(95)06177-0
Dubrulle F, Chaton V, Risoud M, Farah H, Charley Q, Vincent C (2020) The round window sign: a sensitive sign to detect perilymphatic fistulae on delayed postcontrast 3D-FLAIR sequence. Eur Radiol 30: 6303-6310. doi: 10.1007/s00330-020-06924-4
Ehmer DR, Jr., Booth T, Kutz JW, Jr., Roland PS (2010) Radiographic diagnosis of trans-stapedial cerebrospinal fluid fistula. Otolaryngol Head Neck Surg 142: 694-8. doi: 10.1016/j.otohns.2009.12.029
Fee GA (1968) Traumatic perilymphatic fistulas. Arch Otolaryngol 88: 477-80. doi: 10.1001/archotol.1968.00770010479005
Ferber-Viart C, Postec F, Duclaux R, Dubreuil C (1998) Perilymphatic fistula following airbag trauma. Laryngoscope 108: 1255-7. doi: 10.1097/00005537-199808000-00033
Fife TD, Giza C (2013) Posttraumatic vertigo and dizziness. Semin Neurol 33: 238-43. doi: 10.1055/s-0033-1354599
Fitzgerald DC (1995) Persistent dizziness following head trauma and perilymphatic fistula. Arch Phys Med Rehabil 76: 1017-20. doi: 10.1016/s0003-9993(95)81041-2
Fitzgerald DC (1996) Perilymphatic fistula in teens and young adults: emphasis on preexisting sensorineural hearing loss. Am J Otol 17: 397-400.
Fitzgerald DC (2001) Perilymphatic fistula and Meniere’s disease. Clinical series and literature review. Ann Otol Rhinol Laryngol 110: 430-6. doi: 10.1177/000348940111000507
Fitzgerald DC, Getson P, Brasseux CO (1997) Perilymphatic fistula: a Washington, DC, experience. Ann Otol Rhinol Laryngol 106: 830-7. doi: 10.1177/000348949710601005
Foster PK (2016) Autologous intratympanic blood patch for presumed perilymphatic fistulas. J Laryngol Otol 130: 1158-1161. doi: 10.1017/S0022215116009580
Fujita T, Kobayashi T, Saito K, Seo T, Ikezono T, Doi K (2019) Vestibule-Middle Ear Dehiscence Tested With Perilymph-Specific Protein Cochlin-Tomoprotein (CTP) Detection Test. Front Neurol 10: 47. doi: 10.3389/fneur.2019.00047
Fukaya T, Nomura Y (1988) Audiological aspects of idiopathic perilymphatic fistula. Acta Otolaryngol Suppl 456: 68-73. doi: 10.3109/00016488809125080
Garg R, Djalilian HR (2009) Intratympanic injection of autologous blood for traumatic perilymphatic fistulas. Otolaryngol Head Neck Surg 141: 294-5. doi: 10.1016/j.otohns.2009.05.024
Gibson WP (1992) Electrocochleography in the diagnosis of perilymphatic fistula: intraoperative observations and assessment of a new diagnostic office procedure. Am J Otol 13: 146-51.
Gibson WP (1993) Spontaneous perilymphatic fistula: electrophysiologic findings in animals and man. Am J Otol 14: 273-7.
Glasscock ME, 3rd, Hart MJ, Rosdeutscher JD, Bhansali SA (1992) Traumatic perilymphatic fistula: how long can symptoms persist? A follow-up report. Am J Otol 13: 333-8.
Gormley PK (1986) Surgical management of labyrinthine fistula with cholesteatoma. J Laryngol Otol 100: 1115-1123. doi: PMID: 3772236
Gunesh RP, Huber AM (2003) Traumatic perilymphatic fistula. Ann Otol Rhinol Laryngol 112: 221-2. doi: 10.1177/000348940311200305
Gyo K, Kobayashi T, Yumoto E, Yanagihara N (1994) Postoperative recurrence of perilymphatic fistulas. Acta Otolaryngol Suppl 514: 59-62. doi: 10.3109/00016489409127561
Hajiioannou JK, Bathala S, Marnane CN (2009) Case of perilymphatic fistula caused by medially displaced tympanostomy tube. J Laryngol Otol 123: 928-30. doi: 10.1017/S0022215108003873
Harvey SA, Millen SJ (1994) Absent round window reflex: possible relation to step-wise hearing loss. Am J Otol 15: 237-42.
Hatano A, Rikitake M, Komori M, Irie T, Moriyama H (2009) Traumatic perilymphatic fistula with the luxation of the stapes into the vestibule. Auris Nasus Larynx 36: 474-8. doi: 10.1016/j.anl.2008.10.003
Haubner F, Rohrmeier C, Koch C, Vielsmeier V, Strutz J, Kleinjung T (2012) Occurence of a round window membrane rupture in patients with sudden sensorineural hearing loss. BMC Ear Nose Throat Disord 12: 14. doi: 10.1186/1472-6815-12-14
Hazell JW, Fraser JG, Robinson PJ (1992) Positional audiometry in the diagnosis of perilymphatic fistula. Am J Otol 13: 263-9.
Healy GB, Friedman JM, DiTroia J (1978) Ataxia and hearing loss secondary to perilymphatic fistula. Pediatrics 61: 238-41.
Heilen S, Lang CP, Warnecke A, Lenarz T, Durisin M (2020) Exploratory tympanotomy in sudden sensorineural hearing loss for the identification of a perilymphatic fistula – retrospective analysis and review of the literature. J Laryngol Otol 134: 501-508. doi: 10.1017/S0022215120000948
House JW, Morris MS, Kramer SJ, Shasky GL, Coggan BB, Putter JS (1991) Perilymphatic fistula: surgical experience in the United States. Otolaryngol Head Neck Surg 105: 51-61. doi: 10.1177/019459989110500108
Kataoka Y, Ikezono T, Fukushima K, Yuen K, Maeda Y, Sugaya A, Nishizaki K (2013) Cochlin-tomoprotein (CTP) detection test identified perilymph leakage preoperatively in revision stapes surgery. Auris Nasus Larynx 40: 422-4. doi: 10.1016/j.anl.2012.08.001
Khoo LS, Tan TY (2011) Traumatic perilymphatic fistula secondary to stapes luxation into the vestibule: a case report. Ear Nose Throat J 90: E28-31. doi: 10.1177/014556131109000515
Kilic E, Genc H, Aydin U, Asik B, Satar B (2017) Variations in otological presentation of lightning strike victims: Clinical report of 3 patients. Ulus Travma Acil Cerrahi Derg 23: 163-166. doi: 10.5505/tjtes.2016.88580
Kim SH, Kazahaya K, Handler SD (2001) Traumatic perilymphatic fistulas in children: etiology, diagnosis and management. Int J Pediatr Otorhinolaryngol 60: 147-53. doi: 10.1016/s0165-5876(01)00485-2
Kimitsuki T, Hara Y, Komune S (2004) Hearing preservation in perilymphatic fistula due to a congenital fistula in an adult. Eur Arch Otorhinolaryngol 261: 133-5. doi: 10.1007/s00405-003-0639-2
Kita AE, Kim I, Ishiyama G, Ishiyama A (2019) Perilymphatic Fistula After Penetrating Ear Trauma. Clin Pract Cases Emerg Med 3: 115-118. doi: 10.5811/cpcem.2019.1.37404
Klokker M, Vesterhauge S (2005) Perilymphatic fistula in cabin attendants: an incapacitating consequence of flying with common cold. Aviat Space Environ Med 76: 66-8.
Kohut RI, Hinojosa R, Thompson JN, Ryu JH (1995a) Idiopathic perilymphatic fistulae: a temporal bone histopathological study. Clinical, surgical and histopathological correlations. Acta Otolaryngol Suppl 520 Pt 1: 225-34. doi: 10.3109/00016489509125235
Kohut RI, Hinojosa R, Thompson JN, Ryu JH (1995b) Idiopathic perilymphatic fistulas. A temporal bone histopathologic study with clinical, surgical, and histopathologic correlations. Arch Otolaryngol Head Neck Surg 121: 412-20. doi: 10.1001/archotol.1995.01890040036006
Kokesh J, Norton SJ, Duckert LG (1994) Effect of perilymphatic fistulas on evoked otoacoustic emissions in the guinea pig. Am J Otol 15: 466-73.
Koksal A, Ayyildiz V, Ogul H, Kantarci M (2022) Case Report of a Patient With Posttraumatic Perilymphatic Fistula. Ear Nose Throat J: 1455613221131302. doi: 10.1177/01455613221131302
Kubo T, Kohno M, Naramura H, Itoh M (1993) Clinical characteristics and hearing recovery in perilymphatic fistulas of different etiologies. Acta Otolaryngol 113: 307-11. doi: 10.3109/00016489309135814
Kuhweide R, van de Steene V, Vlaminck S, Casselman JW (2007) Reparative granuloma related to perilymphatic fistula. Adv Otorhinolaryngol 65: 296-299. doi: 10.1159/000098845
Kvestad E, Kvaerner KJ, Mair IW (2001) Labyrinthine fistula detection: the predictive value of vestibular symptoms and computerized tomography. Acta Otolaryngol 121: 622-626. doi: PMID: 11583397
Lee JS, Kwon SY, Kim JH, Kim HJ (2015) Bilateral Sequential Pneumolabyrinth Resulting from Nose Blowing. J Audiol Otol 19: 182-5. doi: 10.7874/jao.2015.19.3.182
Lee K, Ochi N, Yamahara K, Makino K, Ikezono T (2020) A Case of Perilymphatic Fistula with Inner Ear Anomaly Diagnosed Preoperatively by the Cochlin-Tomoprotein Detection Test. Case Rep Otolaryngol 2020: 9476915. doi: 10.1155/2020/9476915
Lehrer JF, Poole DC, Sigal B (1980) Use of the glycerin test in the diagnosis of post-traumatic perilymphatic fistulas. Am J Otolaryngol 1: 207-10. doi: 10.1016/s0196-0709(80)80090-1
Lehrer JF, Rubin RC, Poole DC, Hubbard JH, Wille R, Jacobs GB (1984) Perilymphatic fistula–a definitive and curable cause of vertigo following head trauma. West J Med 141: 57-60.
Lollis SS, Weider DJ, Phillips JM, Roberts DW (2006) Ventriculoperitoneal shunt insertion for the treatment of refractory perilymphatic fistula. J Neurosurg 105: 1-5. doi: 10.3171/jns.2006.105.1.1
Magliulo G, Terranova G, Varacalli S, Sepe C (1997) Labyrinthine fistula as a complication of cholesteatoma. Am J Otol 18: 697-701. doi: PMID: 9391663
Maitland CG (2001) Perilymphatic fistula. Curr Neurol Neurosci Rep 1: 486-91. doi: 10.1007/s11910-001-0111-x
Markou K, Rachovitsas D, Veros K, Tsiropoulos G, Tsalighopoulos M, Psillas G (2014) Perilymphatic fistula of the round window after whiplash injury: another cause of inner ear conductive hearing loss. Am J Otolaryngol 35: 822-5. doi: 10.1016/j.amjoto.2014.06.016
Matsuda H, Sakamoto K, Matsumura T, Saito S, Shindo S, Fukushima K, Nishio SY, Kitoh R, Shibasaki O, Ito A, Araki R, Usami SI, Suzuki M, Ogawa K, Hasegawa T, Hagiwara Y, Kase Y, Ikezono T (2017) A nationwide multicenter study of the Cochlin tomo-protein detection test: clinical characteristics of perilymphatic fistula cases. Acta Otolaryngol 137: S53-S59. doi: 10.1080/00016489.2017.1300940
McCabe BF (1984) Labyrinthine fistula in chronic mastoiditis. Ann Otol Rhinol Laryngol Suppl 112: 138-141. doi: PMID: 6431874
McGhee MA, Dornhoffer JL (2000) A case of barotrauma-induced pneumolabyrinth secondary to perilymphatic fistula. Ear Nose Throat J 79: 456-9.
Meyerhoff WL (1993) Spontaneous perilymphatic fistula: myth or fact. Am J Otol 14: 478-81. doi: 10.1097/00129492-199309000-00012
Michel O, Petereit H, Klemm E, Walther LE, Bachmann-Harildstad G (2005) First clinical experience with beta-trace protein (prostaglandin D synthase) as a marker for perilymphatic fistula. J Laryngol Otol 119: 765-9. doi: 10.1258/002221505774481228
Modugno GC, Magnani G, Brandolini C, Savastio G, Pirodda A (2006) Could vestibular evoked myogenic potentials (VEMPs) also be useful in the diagnosis of perilymphatic fistula? Eur Arch Otorhinolaryngol 263: 552-5. doi: 10.1007/s00405-006-0008-z
Morris MS (1994) Perilymphatic fistula with no visible leak of fluid into the middle ear: a new method of intraoperative diagnosis using electrocochleography. Am J Otol 15: 695.
Morris MS, Kil J, Carvlin MJ (1993) Magnetic resonance imaging of perilymphatic fistula. Laryngoscope 103: 729-33. doi: 10.1288/00005537-199307000-00004
Morvan JB, Gempp E, Riviere D, Louge P, Vallee N, Verdalle P (2016) Perilymphatic fistula after underwater diving: a series of 11 cases. Diving Hyperb Med 46: 72-5.
Nakashima T, Sone M, Teranishi MA, Tominaga M, Sugiura M, Naganawa S (2003) Imaging of a congenital perilymphatic fistula. Int J Pediatr Otorhinolaryngol 67: 421-5. doi: 10.1016/s0165-5876(02)00397-x
Nishiike S, Hyo Y, Fukushima H (2008) Stapediovestibular dislocation with pneumolabyrinth. J Laryngol Otol 122: 419-21. doi: 10.1017/S0022215107008171
Ogawa K, Kanzaki J, Ogawa S, Tsuchihashi N, Inoue Y, Yamamoto M (1994) Endoscopic diagnosis of idiopathic perilymphatic fistula. Acta Otolaryngol Suppl 514: 63-5. doi: 10.3109/00016489409127562
Omichi R, Kariya S, Maeda Y, Nishizaki K (2018) Transcanal endoscopic ear surgery for perilymphatic fistula after electric acoustic stimulation. Auris Nasus Larynx 45: 657-660. doi: 10.1016/j.anl.2017.10.004
Osetinsky LM, Hamilton GS, 3rd, Carlson ML (2017) Sport Injuries of the Ear and Temporal Bone. Clin Sports Med 36: 315-335. doi: 10.1016/j.csm.2016.11.005
Palva T, Ramsay H (1989) Treatment of labyrinthine fistula. Arch Otolaryngol Head Neck Surg 115: 804-806. doi: PMID: 2736091
Pappas DG, Simpson LC, Godwin GH (1988) Perilymphatic fistula in children with preexisting sensorineural hearing loss. Laryngoscope 98: 507-10. doi: 10.1288/00005537-198805000-00006
Pashley NR, Shapiro R (1978) Spontaneous perilymphatic fistula. J Otolaryngol 7: 110-8.
Poe DS, Bottrill ID (1994) Comparison of endoscopic and surgical explorations for perilymphatic fistulas. Am J Otol 15: 735-8.
Poe DS, Rebeiz EE, Pankratov MM (1992) Evaluation of perilymphatic fistulas by middle ear endoscopy. Am J Otol 13: 529-33.
Prenzler NK, Schwab B, Kaplan DM, El-Saied S (2018) The role of explorative tympanotomy in patients with sudden sensorineural hearing loss with and without perilymphatic fistula. Am J Otolaryngol 39: 46-49. doi: 10.1016/j.amjoto.2017.10.006
Prisman E, Ramsden JD, Blaser S, Papsin B (2011) Traumatic perilymphatic fistula with pneumolabyrinth: diagnosis and management. Laryngoscope 121: 856-9. doi: 10.1002/lary.21439
Pullen FW, 2nd (1992) Perilymphatic fistula induced by barotrauma. Am J Otol 13: 270-2.
Pyykko I, Selmani Z, Zou J (2012) Low-frequency sound pressure and transtympanic endoscopy of the middle ear in assessment of “spontaneous” perilymphatic fistula. ISRN Otolaryngol 2012: 137623. doi: 10.5402/2012/137623
Qureshi HA, Zeitler DM (2021) Intratympanic Steroid Injection Complicated by Iatrogenic Perilymphatic Fistula: A Cautionary Tale. Laryngoscope 131: 2088-2090. doi: 10.1002/lary.29613
Rawal R, Zhao X, Lipson S, J RB (2021) Endoscopic Repair of Traumatic Perilymphatic Fistula in Children: A Case Series. J Int Adv Otol 17: 182-185. doi: 10.5152/JIAO.2021.8390
Reilly JS (1989) Congenital perilymphatic fistula: a prospective study in infants and children. Laryngoscope 99: 393-7. doi: 10.1288/00005537-198904000-00006
Reilly JS, Kenna MA (1989) Congenital perilymphatic fistula: an overlooked diagnosis? Am J Otol 10: 496-8. doi: 10.1097/00129492-198911000-00018
Ruben RJ, Yankelowitz SM (1989) Spontaneous perilymphatic fistula in children. Am J Otol 10: 198-207.
Sass K, Densert B, Magnusson M (1997) Transtympanic electrocochleography in the assessment of perilymphatic fistulas. Audiol Neurootol 2: 391-402. doi: 10.1159/000259264
Sekula J, Wlodyka J (1982) The round window in acute hearing loss. Audiology 21: 55-60.
Selmani Z, Ishizaki H, Pyykko I (2004) Can low frequency sound stimulation during posturography help diagnosing possible perilymphatic fistula in patients with sensorineural hearing loss and/or vertigo? Eur Arch Otorhinolaryngol 261: 129-32. doi: 10.1007/s00405-003-0614-y
Selmani Z, Pyykko I, Ishizaki H, Marttila TI (2002) Role of transtympanic endoscopy of the middle ear in the diagnosis of perilymphatic fistula in patients with sensorineural hearing loss or vertigo. ORL J Otorhinolaryngol Relat Spec 64: 301-6. doi: 10.1159/000066074
Shepard NT, Telian SA, Niparko JK, Kemink JL, Fujita S (1992) Platform pressure test in identification of perilymphatic fistula. Am J Otol 13: 49-54.
Sheridan MF, Hetherington HH, Hull JJ (1999) Inner ear barotrauma from scuba diving. Ear Nose Throat J 78: 181, 184, 186-7 passim.
Shupak A (2006) Recurrent diving-related inner ear barotrauma. Otol Neurotol 27: 1193-6. doi: 10.1097/01.mao.0000231499.69404.22
Skedros DG, Cass SP, Hirsch BE, Kelly RH (1993) Sources of error in use of beta-2 transferrin analysis for diagnosing perilymphatic and cerebral spinal fluid leaks. Otolaryngol Head Neck Surg 109: 861-4. doi: 10.1177/019459989310900514
Smith M, Darrat I, Seidman M (2012) Otologic complications of cotton swab use: one institution’s experience. Laryngoscope 122: 409-11. doi: 10.1002/lary.22437
Sun GH, Simons JP, Mandell DL (2006) Bilateral perilymphatic fistulas from a lightning strike: a case report. Laryngoscope 116: 1039-42. doi: 10.1097/01.MLG.0000217648.90799.B5
Suzuki M, Kitajima N, Ushio M, Shintani M, Ishibashi T (2003) Changes in the Tullio phenomenon and the fistula sign in the course of endolymphatic hydrops. ORL J Otorhinolaryngol Relat Spec 65: 125-8.
Tsubota M, Shojaku H, Watanabe Y (2009) Prognosis of inner ear function in pneumolabyrinth: case report and literature review. Am J Otolaryngol 30: 423-6. doi: 10.1016/j.amjoto.2008.07.010
Tsunoda A, Anzai T, Matsumoto F, Ikeda K, Tsunoda R (2021) A case of perilymphatic fistula caused by surgical drilling with preserved normal hearing. Am J Otolaryngol 42: 102753. doi: 10.1016/j.amjoto.2020.102753
Venkatasamy A, Al Ohraini Z, Karol A, Karch-Georges A, Riehm S, Rohmer D, Charpiot A, Veillon F (2020) CT and MRI for the diagnosis of perilymphatic fistula: a study of 17 surgically confirmed patients. Eur Arch Otorhinolaryngol 277: 1045-1051. doi: 10.1007/s00405-020-05820-3
Weber PC, Bluestone CD, Kenna MA, Kelley RH (1995) Correlation of beta-2 transferrin and middle ear abnormalities in congenital perilymphatic fistula. Am J Otol 16: 277-82.
Weber PC, Bluestone CD, Perez B (2003) Outcome of hearing and vertigo after surgery for congenital perilymphatic fistula in children. Am J Otolaryngol 24: 138-42. doi: 10.1016/s0196-0709(02)32418-9
Weber PC, Kelly RH, Bluestone CD, Bassiouny M (1994) Beta 2-transferrin confirms perilymphatic fistula in children. Otolaryngol Head Neck Surg 110: 381-6. doi: 10.1177/019459989411000405
Weber PC, Perez BA, Bluestone CD (1993) Congenital perilymphatic fistula and associated middle ear abnormalities. Laryngoscope 103: 160-4. doi: 10.1002/lary.5541030207
Weider DJ (1997) Tinnitus: Report of Ten Cases of Perilymphatic Fistula and/or Endolymphatic Hydrops Improved by Surgery. Int Tinnitus J 3: 11-21.
Weider DJ, Roberts DW, Phillips J (2005) Ventriculoperitoneal shunt as treatment for perilymphatic fistula: a report of six cases. Int Tinnitus J 11: 137-45.
Weinreich HM, Carey JP (2019) Perilymphatic Fistulas and Superior Semi-Circular Canal Dehiscence Syndrome. Adv Otorhinolaryngol 82: 93-100. doi: 10.1159/000490276
Weissman JL, Weber PC, Bluestone CD (1994) Congenital perilymphatic fistula: computed tomography appearance of middle ear and inner ear anomalies. Otolaryngol Head Neck Surg 111: 243-9. doi: 10.1177/01945998941113P113
Whitelaw AS, Young I (2005) A case of perilymphatic fistula in blunt head injury. Emerg Med J 22: 921. doi: 10.1136/emj.2004.020495
Yanagihara N, Nishioka I (1987) Pneumolabyrinth in perilymphatic fistula: report of three cases. Am J Otol 8: 313-8.
Yaniv E, Hacking D, Ziv-El L (1986) Perilymphatic fistulas: are they exclusive to the round and oval windows? Laryngoscope 96: 360-2. doi: 10.1288/00005537-198604000-00004
Yaniv E, Hacking DP (1987) Combined perilymphatic fistulas of the round window and lateral semicircular canal. A report of 2 cases. S Afr Med J 71: 391-2.
![]()