By Marcello Cherchi, MD PhD
For patients
The cause of scleroderma (also called systemic sclerosis) is unknown. This disease causes thickening of tissues in organs such as the skin, stomach/intestines, lungs, kidneys, brain and nerves. Occasionally patients with scleroderma will develop hearing loss, tinnitus or disequilibrium. In such cases your doctor may check some tests to be sure that those symptoms are not coming from some other more common disease. There is no cure for scleroderma, but when scleroderma seems to be the cause of those symptoms, it is reasonable to talk with an audiologist or vestibular physical therapist.
For clinicians
Overview
Scleroderma, also called systemic sclerosis, is a rare multi-system connective tissue disease of unknown etiology. Some scleroderma patients complain of audiologic symptoms (hearing loss, tinnitus) and/or vestibular symptoms. Given the rarity of scleroderma, in some cases these symptoms may be due to more common diseases that happen to be coincident with scleroderma, while in other cases these deficits may truly be the result of scleroderma itself. If no other cause is found, then referral to audiology and/or vestibular rehabilitation therapy is medically reasonable. The management of scleroderma is usually supervised by a rheumatologist.
Introduction
Scleroderma, also called systemic sclerosis, is a rare connective tissue disease of unknown etiology in which proliferative vascular lesions involving microvessels and small arteries result in collagen deposition and fibrosis in multiple organ systems, including the skin, gastrointestinal tract, lungs, kidneys, and less commonly the nervous system. Raynaud’s phenomenon is sometimes the harbinger of scleroderma. Broad categories of scleroderma include diffuse systemic sclerosis and localized systemic sclerosis, the latter of which has lesser visceral involvement. Some patients with scleroderma develop hearing loss beyond what is expected for age; this hearing loss can be unilateral, bilateral (symmetric or asymmetric), sensorineural or mixed, gradual or abrupt. Scleroderma patients can also exhibit abnormalities on vestibular testing (such as on various ocular motor tests and static posturography), and can develop benign paroxysmal positional vertigo.
Epidemiology
Scleroderma is rare, with a reported annual incidence of 4 to 12 per 1 million individuals. It is more common among individuals aged 30 – 50 years (Rabelo and Corona 2014). Scleroderma affects women three (Rabelo and Corona 2014) to four (Choi et al. 2012) times more frequently than men.
Genetics
The genetics of scleroderma are unknown. Most data implicate loci in the major histocompatibility complex and fibrillin-1, but other candidates include mutations in genes encoding for angiotensin converting enzyme, nitric oxide synthase, CD19 and PTPN22.
Pathophysiological mechanism of disease
Scleroderma is a connective tissue disease of unknown etiology. Pathologically it is characterized by marked by proliferative vascular lesions involving small arteries and microvessels (Amor-Dorado et al. 2008a), collagen deposition in multiple organ systems (Abou-Taleb and Linthicum 1987) and diffuse connective tissue fibrosis that can involve the skin, gastrointestinal tract, lungs, heart and kidneys (Amor-Dorado et al. 2008a), and less commonly the central and peripheral nervous systems. Proposed pathophysiological mechanisms have included, “endothelial dysfunction, fibroblast dysfunction, and dysregulation of the immune system” (Amor-Dorado et al. 2008a).
The mechanism by which scleroderma specifically causes audiologic and vestibular problems is unknown. Given the histopathologic changes described in a temporal bone study by Abou-Taleb and Linthicum (Abou-Taleb and Linthicum 1987), Deroee and colleagues (Deroee et al. 2009) speculate, “It is possible that decreased blood flow due to vasculitis is the cause of hearing loss,” a theory also suggested by Rabelo and colleagues (Rabelo and Corona 2014). Contrastingly, Santarelli and colleagues (Santarelli et al. 2006) suggest that auditory neuropathy may be the mechanism of hearing loss in scleroderma.
Clinical presentation
Raynaud’s phenomenon is sometimes the initial manifestation of a disease process that eventually declares itself as scleroderma (Abou-Taleb and Linthicum 1987)
Amor-Dorado and colleagues (Amor-Dorado et al. 2008a) studied 27 scleroderma patients and reported that 19 (54%) complained of hearing loss.
Berrettini and colleagues (Berrettini et al. 1994) studied 37 scleroderma patients and found that 23 (62%) reported audiologic or vestibular complaints. Of those 23 patients, 11 (48%) complained of exclusively of auditory symptoms (hearing loss or tinnitus), 4 (17%) complained exclusively of vestibular symptoms, and 8 (35%) complained of both auditory and vestibular symptoms.
Salvador and colleagues (Salvador et al. 2025) conducted a systematic review and meta-analysis of 13 studies that included 414 scleroderma patients and 390 control subjects. They reported that scleroderma patients presented with tinnitus at 34.1%, vertigo at 32.4% and subjective hearing loss at 20.8% higher than control subjects.
Deroee and colleagues (Deroee et al. 2009) reported the case of a 65 year old man with scleroderma who suffered sudden sensorineural hearing loss bilaterally.
Testing: audiologic
On audiometry the hearing loss in scleroderma can be unilateral, bilateral (symmetric or asymmetric), sensorineural, conductive or mixed, suggesting that both the inner ear and the middle ear can be affected.
Berrettini and colleagues (Berrettini et al. 1994) studied audiometry in 37 scleroderma patients and reported that 14 (38%) showed hearing loss. Of the 14 patients with hearing loss, only 1 (7%) had unilateral hearing loss, while the remaining 13 (93%) had bilateral hearing loss. Of the 14 patients with hearing loss, it was sensorineural in 10 (71%) and mixed in 4 (29%).
Kastanioudakis and colleagues (Kastanioudakis et al. 2001) studied audiometry in 30 scleroderma patients and reported sensorineural hearing loss in 6 (20%) and mixed hearing loss in 1 (3%).
Amor-Dorado and colleagues (Amor-Dorado et al. 2008a) studied 35 scleroderma patients (limited systemic sclerosis) and reported that 27 (77%) showed hearing loss (beyond what was expected for age) on audiometry. Of these 27 patients with unexpected hearing loss, 24 (89%) had sensorineural hearing loss which was symmetrical in 13 patients and asymmetrical in 11. Of the 27 patients with unexpected hearing loss, 3 (11%) had mixed (sensorineural and conductive) hearing loss. They also reported that scleroderma patients had abnormal tympanograms and stapedius reflexes compared to healthy controls.
Testing: vestibular
Rabelo and colleagues (Rabelo and Corona 2014) conducted a systematic literature review and found that studies reported vestibular abnormalities ranging from 11% to 63%, and that “the most common findings were changes in caloric testing, positional nystagmus, abnormal oculocephalic reflex, changes in clinical tests of sensory integration, and benign paroxysmal positional vertigo.”
Amor-Dorado and colleagues (Amor-Dorado et al. 2008b) reported that 7 (17%) of 41 scleroderma patients exhibited oculographic abnormalities on vestibular testing. They further commented that the ocular motor findings were compatible with posterior canal benign paroxysmal positional vertigo in 2 scleroderma patients, and findings compatible with lateral canal benign paroxysmal positional vertigo in 5 scleroderma patients. Choi and colleagues (Choi et al. 2012) also reported a case of a scleroderma patient with direction changing positional nystagmus compatible with lateral canal benign paroxysmal positional vertigo.
Berrettini and colleagues (Berrettini et al. 1994) conducted vestibular tests in 37 scleroderma patients and reported that 4 (11%) exhibited some abnormality. Of these, 2 exhibited positional nystagmus, 1 exhibited a “marked unilateral compensated vestibular deficit) and 1 exhibited bilateral caloric weakness.
Amor-Dorado and colleagues (Amor-Dorado et al. 2008a) reported that of 34 scleroderma patients who underwent vestibular testing, 10 (29%) exhibited abnormalities in the oculo-cephalic reflex, 9 (26%) exhibited head shaking nystagmus, 3 (9%) exhibited positional nystagmus in at least 3 positions, and 11 (31%) exhibited abnormal caloric asymmetry.
Amor-Dorado and colleagues (Amor-Dorado et al. 2008a) reported that 16 (46%) out of 34 scleroderma patients exhibited abnormalities on static posturography (“foam and dome test”). Similarly, Amor-Dorado and colleagues (Amor-Dorado et al. 2008b) reported that 20 (48%) of 42 scleroderma patients exhibited abnormalities on static posturography.
Testing: other
Some investigators report the finding of a patulous Eustachian tube in scleroderma patients (Deroee et al. 2009; Kastanioudakis et al. 2001).
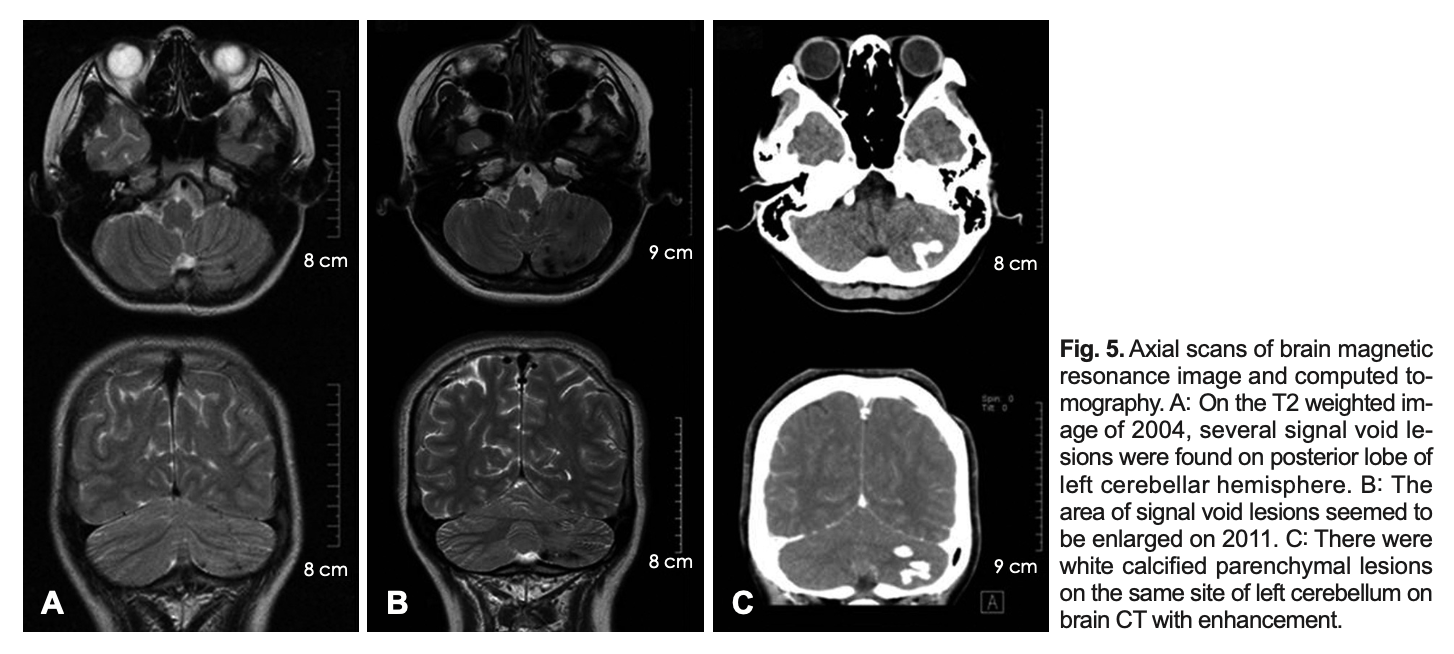
Imaging
Scleroderma can cause intraparenchymal brain calcifications.
The Figure below, from Choi and colleagues (Choi et al. 2012), shows an example of intracerebral calcification particularly involving the left cerebellar hemisphere.
Histopathology
Few temporal bone reports are available in patients with scleroderma. Abbou-Taleb and Linthicum (Abou-Taleb and Linthicum 1987) describe:
“The blood vessels in the stria [vascularis of the cochlea] were larger than normal and there was focal strial atrophy. The number of outer hair cells, dendrites, and ganglion cells was reduced by about 50 per cent in the area from the anterior basal turn to the hook. Blood vessels around the endolymphatic sac and in the internal auditory canal, mastoid cells, and bone marrow spaces had thickened walls and hyalinization. Perivascular fibrosis surrounded small arterioles and venules in some areas with a few ghost vessels. The amount of thickening of blood vessels around the ELS [endolymphatic sac] and the IAC [internal auditory canal] was approximately the same. There was no evidence of new bone formation or of hydrops” (Abou-Taleb and Linthicum 1987).
Differential diagnosis
The clinical history of the auditory and vestibular symptoms, and the abnormalities reported on audiologic and vestibular testing, are neither specific nor sensitive for scleroderma. Given its rarity, if a scleroderma patient reports audiologic or vestibular symptoms, it is medically reasonable to undertake a screening audiologic and vestibular workup to seek more common causes of these symptoms.
Treatment and prognosis
Scleroderma is usually managed by a rheumatologist.
Since the underlying cause of scleroderma is unknown, management is supportive rather than curative. As far as audiologic and vestibular symptoms are concerned, if a screening workup reveals no evidence for a more convincing explanation, then referral to audiology and/or vestibular rehabilitation therapy is medically reasonable.
References
Abou-Taleb A, Linthicum FH, Jr. (1987) Scleroderma and hearing loss: (histopathology of a case). J Laryngol Otol 101: 656-62. doi: 10.1017/s0022215100102476
Amor-Dorado JC, Arias-Nunez MC, Miranda-Filloy JA, Gonzalez-Juanatey C, Llorca J, Gonzalez-Gay MA (2008a) Audiovestibular manifestations in patients with limited systemic sclerosis and centromere protein-B (CENP-B) antibodies. Medicine (Baltimore) 87: 131-141. doi: 10.1097/MD.0b013e318173aa56
Amor-Dorado JC, Barreira-Fernandez MP, Arias-Nunez MC, Gomez-Acebo I, Llorca J, Gonzalez-Gay MA (2008b) Benign paroxysmal positional vertigo and clinical test of sensory interaction and balance in systemic sclerosis. Otol Neurotol 29: 1155-61. doi: 10.1097/MAO.0b013e31818a086e
Berrettini S, Ferri C, Pitaro N, Bruschini P, Latorraca A, Sellari-Franceschini S, Segnini G (1994) Audiovestibular involvement in systemic sclerosis. ORL J Otorhinolaryngol Relat Spec 56: 195-8. doi: 10.1159/000276655
Choi EJ, Lee DW, Park CW, Lee SH (2012) A case of linear scleroderma involving cerebellum with vertigo. Korean J Audiol 16: 87-90. doi: 10.7874/kja.2012.16.2.87
Deroee AF, Huang TC, Morita N, Hojjati M (2009) Sudden hearing loss as the presenting symptom of systemic sclerosis. Otol Neurotol 30: 277-9. doi: 10.1097/MAO.0b013e31819bda52
Kastanioudakis I, Ziavra N, Politi EN, Exarchakos G, Drosos AA, Skevas A (2001) Hearing loss in progressive systemic sclerosis patients: a comparative study. Otolaryngol Head Neck Surg 124: 522-5. doi: 10.1067/mhn.2001.115092
Rabelo MB, Corona AP (2014) Auditory and vestibular dysfunctions in systemic sclerosis: literature review. Codas 26: 337-42. doi: 10.1590/2317-1782/20140201475
Salvador CD, Keith BA, Ward C, Nguyen SA, Gordis T, Chidarala S, Brennan E, Rizk H (2025) Audiovestibular symptoms in systemic sclerosis: a systematic review and meta-analysis. Eur Arch Otorhinolaryngol 282: 1147-1157. doi: 10.1007/s00405-024-09001-4
Santarelli R, Scimemi P, Dal Monte E, Genovese E, Arslan E (2006) Auditory neuropathy in systemic sclerosis: a speech perception and evoked potential study before and after cochlear implantation. Eur Arch Otorhinolaryngol 263: 809-15. doi: 10.1007/s00405-006-0075-1
![]()