By Marcello Cherchi, MD PhD
For patients
West Nile virus (WNV) infections in humans usually occur in July – September. In rare cases, WNV may affect the nervous system, and sometimes cause disequilibrium. If you have been diagnosed with WNV and experience disequilibrium, then your doctor may consider checking several tests of inner ear and balance function.
For clinicians
Overview
West Nile virus (WNV) is transmitted from birds to humans primarily by mosquitoes. Infection is more likely to occur in July – September. Most infected people are asymptomatic, though 20% can have moderate symptoms, and 0.7% can get neuroinvasive disease (meningitis, encephalitis, flaccid paralysis). Among patients with neuroinvasive disease (usually encephalitis), 31% of patients experience “ataxia” and 14% experience “vertigo.” The mechanisms for these symptoms of disequilibrium are unclear, but candidates include vestibular weakness and acquired periodic alternating nystagmus (PAN). Treatment is supportive.
Introduction
West Nile virus (WNV) is an enveloped positive-stranded ribonucleic acid virus belonging to the Flaviviridiae family. It is an arbovirus (arthropod-borne), transmitted to humans primarily through the vector of mosquitoes (less commonly by ticks) from birds (the reservoir host).
The virus was first isolated from a patient in the West Nile province of Uganda in 1937. WNV is found in Africa, Western Asia, Southern and Western Europe and in the Americas. It is the leading cause of arboviral disease in the continental United States. The WNV outbreak in the United States in 2002 was the largest outbreak of arboviral disease ever recorded in the Western Hemisphere.
Most individuals infected with WNV are asymptomatic. About 20% of infected individuals develop moderate symptoms such as fever, neck stiffness, headache, body ache, arthralgias, myalgias, nausea, vomiting, rash, swollen glands and fatigue. About 0.7% of patients develop neuroinvasive disease, manifesting with meningitis, encephalitis (which can be fatal) or flaccid paralysis.
Epidemiology
WNV tends to spread during spring and autumn, corresponding with the migratory patterns of its reservoir host (birds); it is more common in July – September. People over the age of 50 years, and immunocompromised individuals, are more vulnerable to developing neuroinvasive disease.
Pathophysiological mechanism of disease
West Nile virus (WNV) is reported to cause “ataxia” in 31% of patients and “vertigo” in 14% of patients (Pepperell et al. 2003).
- The “ataxia” is often ascribed to cerebellar dysfunction (in cases of encephalitis).
- The mechanism of “vertigo” is unclear; “WNV vestibular neuritis” is plausible — given that WNV is documented to cause other cranial neuropathies (Al-Hashimi and Okon 2024; Anninger et al. 2003; Ayça et al. 2021; Cunha et al. 2006; Gilad et al. 2003; Hart et al. 2014; Koevary 2005; Rosenheck et al. 2022; Ross and Worthington 2004; Vaispapir et al. 2002) — but unproven.
We have examined a patient who suffered WNV encephalitis who had different patterns of vestibular weakness on each side. Specifically:
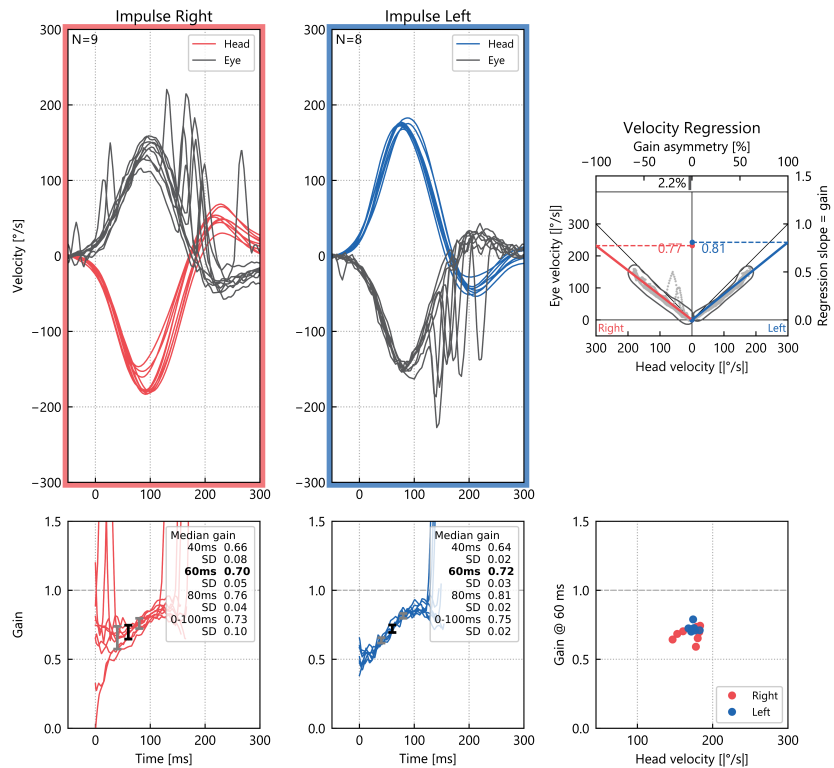
- Bilateral vestibular weakness involving horizontal semicircular canal afferents was identified on video head impulse testing (vHIT) as shown in Figure 1.
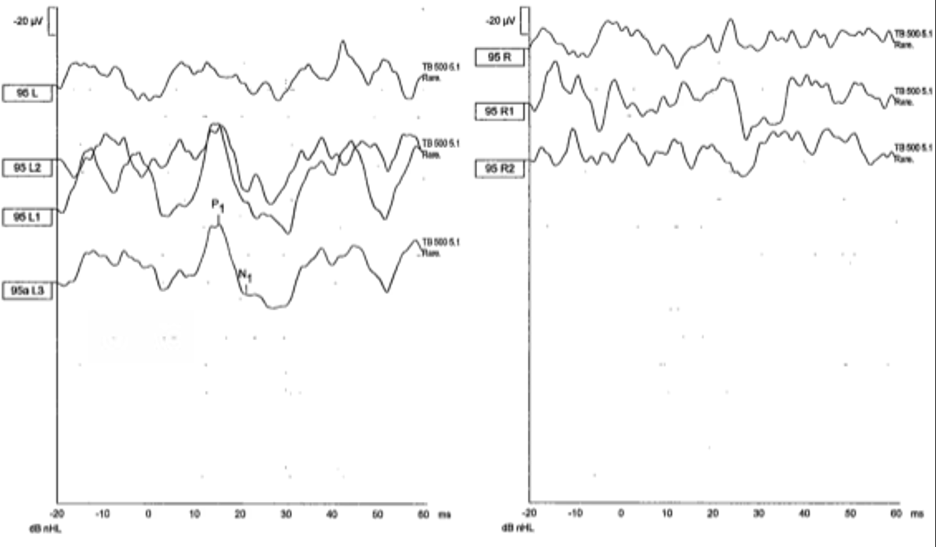
- Right-sided vestibular weakness involving saccular afferents was identified on cervical vestibular evoked myogenic potentials (cVEMP) as shown in Figure 2.
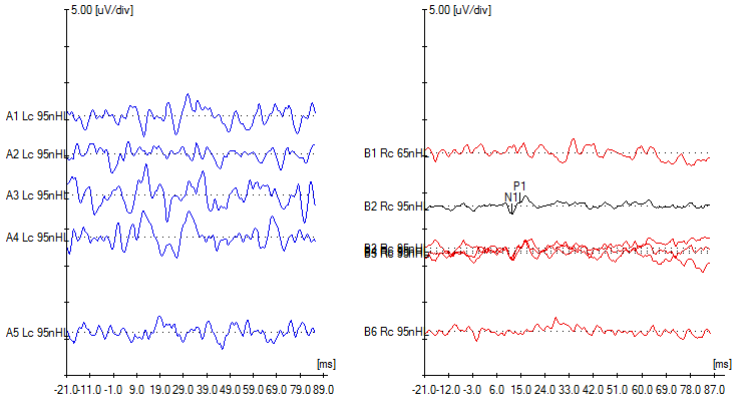
- Left-sided vestibular weakness involving utricular afferents was identified on ocular vestibular evoked myogenic potentials (oVEMP) as showing in Figure 3.
This same patient also exhibited periodic alternating nystagmus (PAN), as shown in Figure 4.
Panel A
Panel B
Panel C
Panel D
Figure 4: Selected videonystagmography tracings demonstrating periodic alternating nystagmus (PAN). In these tracings of horizontal eye movements, by convention an upward deflection represents a rightward eye movement, and a downward deflection represents a leftward eye movement; the red tracing represents the right eye, and the blue tracing represents the left eye; the numbers along the horizontal axis of the tracing are the number of seconds since the start of the recording; the numbers along the vertical axis of each tracing represent the deflection (in degrees) of the eye from the center (primary position of gaze). Panel A shows spontaneous nystagmus, initially right beat. Panel B shows that around 115 seconds the spontaneous right beat nystagmus ceased, and by about 140 seconds had shifted to spontaneous left beat nystagmus. Panel C shows crescendoing of the left beat nystagmus. Panel D shows that around 240 seconds the left beat nystagmus subsided, and by around 255 seconds began to shift back to right beat nystagmus
Acquired PAN has been observed in other encephalidites (Baloh et al. 1976), but as far as we are aware, it has not been previously reported in association with WNV encephalitis.
Thus, while it remains unclear how WNV can cause disequilibrium, the case presented above suggests that candidate mechanisms include:
- Cranial neuropathy — basically, vestibular neuritis (VN) perhaps from WNV itself. Another potential mechanism would be damage to the vestibular nuclei from brainstem encephalitis.
- Acquired periodic alternating nystagmus (PAN), presumably from brainstem encephalitis.
Testing: vestibular
Given the candidate mechanisms described earlier, in WNV patients suffering from disequilibrium, it is medically reasonable to consider checking:
- Tests that would identify vestibular weakness, such as cervical vestibular evoked myogenic potentials (cVEMP), ocular vestibular evoked myogenic potentials (oVEMP), video head impulse testing (vHIT) and rotatory chair testing (RCT).
- Instrumented ocular motortesting (such as videonystagmography), in order to assess for periodic alternating nystagmus (PAN).
- In PAN is absent, then caloric testing is also reasonable. (If PAN is present, then this will make the results of caloric testing difficult to interpret.)
Testing: other
Acute WNV infection can be detected on MAC-ELISA (IgM antibody capture enzyme-linked immunosorbent assay) on serum or cerebrospinal fluid. In some cases diagnosis may need to be confirmed by plaque reduction neutralization (PRNT). If a patient is immunocompromised, then direct detection of the virus itself can be undertaken with reverse transcription polymerase chain reaction (RT-PCR).
Imaging
Most WNV patients referred to an otoneurology or neuro-otology clinic will already have had brain imaging performed. If this has not been done, then it is sensible to check MRI of the brain and internal auditory canals without and with contrast.
Treatment
There is no direct treatment for WNV infection, so management is supportive.
If workup identifies vestibular weakness, than referral to vestibular rehabilitation therapy (VRT) is reasonable.
Pharmacologic management of period alternating nystagmus (PAN) — such as with baclofen (DiBartolomeo and Yee 1988; Halmagyi et al. 1980; Isago et al. 1985) — can be considered, though this has not been studied specifically in the context of WNV encephalitis.
References
Al-Hashimi I, Okon E (2024) West Nile Virus: A Neglected Cause of Bell’s Palsy? Cureus 16: e62486. doi: 10.7759/cureus.62486
Anninger WV, Lomeo MD, Dingle J, Epstein AD, Lubow M (2003) West Nile virus-associated optic neuritis and chorioretinitis. Am J Ophthalmol 136: 1183-5. doi: 10.1016/s0002-9394(03)00738-4
Ayça S, Akkoç G, Özdemir H, Selçuk-Duru HN (2021) An unusual neurologic presentation of pediatric neuroinvasive West Nile virus infection: ophthalmoplegia. Turk J Pediatr 63: 909-912. doi: 10.24953/turkjped.2021.05.019
Baloh RW, Honrubia V, Konrad HR (1976) Periodic alternating nystagmus. Brain 99: 11-26. doi: 10.1093/brain/99.1.11
Cunha BA, Eisenstein LE, Wirkowski E, Klein NH, Johnson DH (2006) West Nile encephalitis relapse presenting with abducens and facial nerve palsies. Am J Med 119: e1-2. doi: 10.1016/j.amjmed.2005.09.061
DiBartolomeo JR, Yee RD (1988) Periodic alternating nystagmus. Otolaryngol Head Neck Surg 99: 552-7. doi: 10.1177/019459988809900603
Gilad R, Lampl Y, Sadeh M, Paul M, Dan M (2003) Optic neuritis complicating west nile virus meningitis in a young adult. Infection 31: 55-6. doi: 10.1007/s15010-002-3039-4
Halmagyi GM, Rudge P, Gresty MA, Leigh RJ, Zee DS (1980) Treatment of periodic alternating nystagmus. Ann Neurol 8: 609-11. doi: 10.1002/ana.410080611
Hart J, Jr., Tillman G, Kraut MA, Chiang HS, Strain JF, Li Y, Agrawal AG, Jester P, Gnann JW, Jr., Whitley RJ (2014) West Nile virus neuroinvasive disease: neurological manifestations and prospective longitudinal outcomes. BMC Infect Dis 14: 248. doi: 10.1186/1471-2334-14-248
Isago H, Tsuboya R, Kataura A (1985) A case of periodic alternating nystagmus: with a special reference to the efficacy of baclofen treatment. Auris Nasus Larynx 12: 15-21
Koevary SB (2005) Ocular involvement in patients infected by the West Nile virus. Optometry 76: 609-12. doi: 10.1016/j.optm.2005.08.015
Pepperell C, Rau N, Krajden S, Kern R, Humar A, Mederski B, Simor A, Low DE, McGeer A, Mazzulli T, Burton J, Jaigobin C, Fearon M, Artsob H, Drebot MA, Halliday W, Brunton J (2003) West Nile virus infection in 2002: morbidity and mortality among patients admitted to hospital in southcentral Ontario. CMAJ 168: 1399-405.
Rosenheck MS, Higham C, Sanzone K, Caprio C (2022) New-onset Bell’s palsy after neuroinvasive West Nile virus. BMJ Case Rep 15. doi: 10.1136/bcr-2022-249770
Ross JJ, Worthington MG (2004) Bilateral sixth nerve palsy in West Nile meningoencephalitis. J Neuroophthalmol 24: 97-8. doi: 10.1097/00041327-200403000-00034
Vaispapir V, Blum A, Soboh S, Ashkenazi H (2002) West Nile virus meningoencephalitis with optic neuritis. Arch Intern Med 162: 606-7. doi: 10.1001/archinte.162.5.606-a
![]()