By Marcello Cherchi, MD PhD
For patients
Mingjia Dai came up with a way of treating mal de debarquement syndrome (MdDs) that does not use medications. Instead it involves looking at moving stripes while rocking the head from side to side.
For clinicians
Overview
Dr. Mingjia Dai hypothesized that mal de debarquement syndrome (MdDs) resulted from maladaptive linking of semicircular canal input with otolith input. He developed a non-pharmacologic treatment intended to unlink these inputs. The technique involves exposing the patient to a horizontally-moving optokinetic stimulus while oscillating the head in the roll plane. Dai and colleagues reported encouraging results at 1 year after treatment.
Introduction
Dr. Mingjia Dai (1948 – 2019) was instrumental in developing a non-pharmacologic treatment protocol for mal de debarquement syndrome (MdDs), building on previous work by Dr. Bernard Cohen, Dr. Theodore Raphan and Dr. David Robinson pertaining to the velocity storage mechanism (Cohen 2019; Dai et al. 1991).
Mechanism
The key hypothesis underlying Dai’s treatment for MdDs was that the disease reflects maladaptive linking of semicircular canal input with otolith input, perhaps localizing to the vestibulocerebellum (Cohen et al. 2018). Dai and colleagues explain:
“The VOR [vestibulo-ocular reflex] is composed of three components: yaw, pitch, and roll. All three are the subject of adaptation. Adaptation of the VOR can occur in a specific context across different axes. Contextual adaptation is long lasting, and the changes induced by 1 h of training can last for several days… [S]imultaneous rotation about yaw and oscillation in roll induces oscillation in pitch. If a subject is adapted to that context, then, similar to cross-axis adaptation, simple oscillation in roll can induce adaptive compensatory eye oscillations in pitch. This finding became the bases for the hypotheses of the underlying mechanism of MdDS” (Dai et al. 2017).
The aim of the treatment is essentially to unlink these inappropriately cross-coupled inputs. The strategy devised by Dai accomplishes this by readaptation of the vestibulo-ocular reflex (Dai et al. 2014). The technique involves exposing the patient to a specific optokinetic visual stimulus (a field of vertically oriented stripes that are moving horizontally at a constant velocity) while the patient’s head is gently oscillated in the roll plane.
This technique is illustrated in the Figure below from Dai and colleagues (Dai et al. 2014).
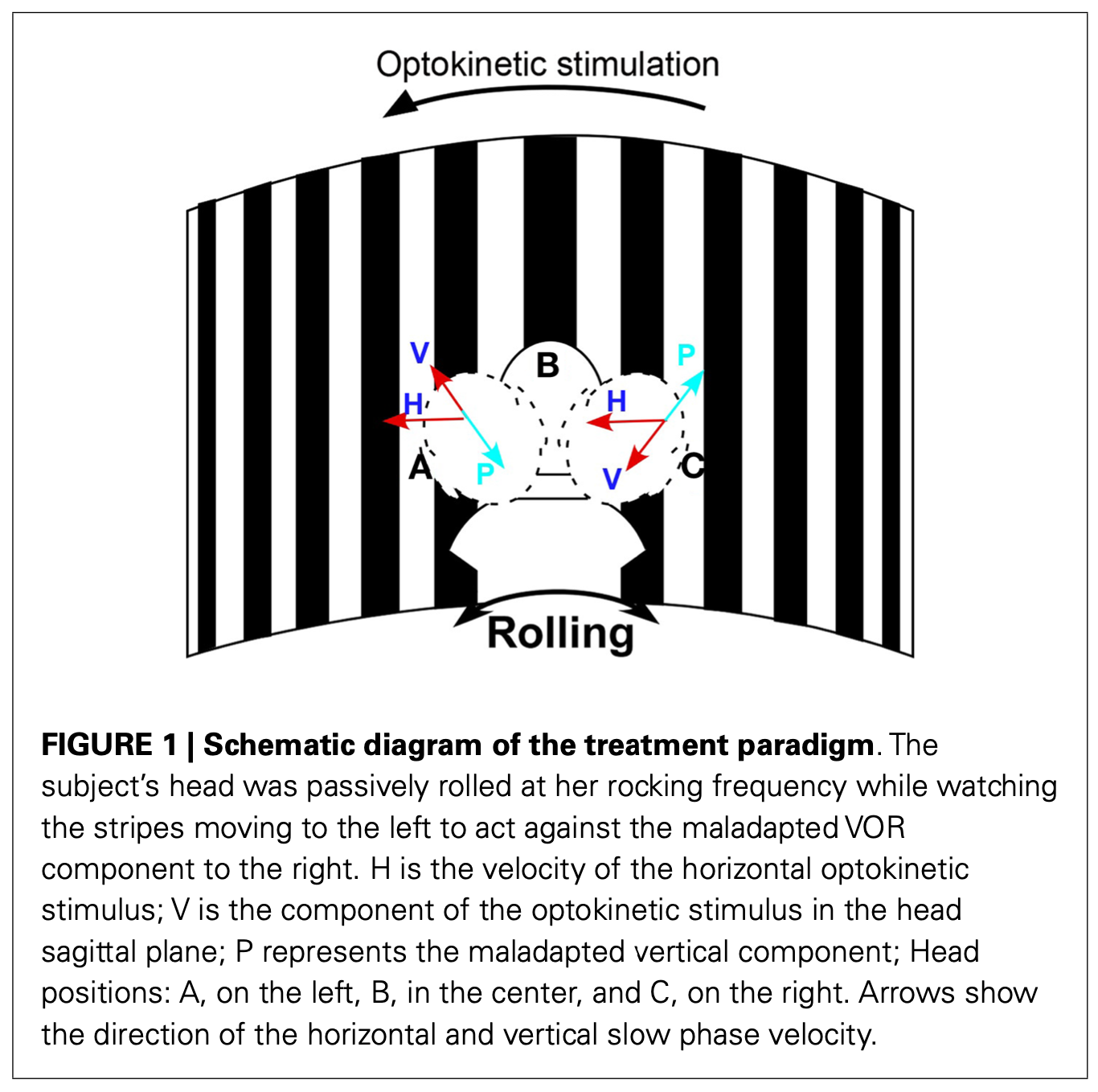
The direction of the optokinetic stimulation is determined by the direction in which the patient turns on the Fukuda-Unterberger stepping test (Dai et al. 2014).
There has been preliminary study on whether this treatment can be delivered through a virtual reality headset (Yakushin et al. 2020).
Outcomes
Dai and colleagues (Dai et al. 2017) treated 141 patients with mal de debarquement syndrome (120 were “classic” cases, and 21 were spontaneously occurring cases). They reported the following results at 1 year after treatment:
“The initial rate of significant improvement after a week of treatment was 78% in classic and 48% in spontaneous patients. One year later, significant improvement was maintained in 52% of classic and 48% of spontaneous subjects. There was complete remission of symptoms in 27% (32) of classic and 19% (4) of spontaneous patients. Although about half of them did not achieve a 50% improvement, most reported fewer and milder symptoms than before. The success of the treatment was generally inversely correlated with the duration of the MdDS symptoms and with the patients’ ages. Prolonged travel by air or car on the way home most likely contributed to the symptomatic reversion from the initial successful treatment” (Dai et al. 2017).
Cautions and contraindications
Keep in mind that mal de debarquement syndrome is rare, and it can (and does) occur in patients suffering from other more common otovestibular disorders. Thus, before embarking on treatment for mal de debarquement it is imperative to exclude other diagnoses (or treat any that are found).
Other notes
To our knowledge, the only institution currently offering this treatment for mal de debarquement syndrome is the laboratory originally spearheaded by Dr. Dai himself at the Mount Sinai Icahn School of Medicine in New York (https://labs.icahn.mssm.edu/dailab/), which is enrolling patients in a study through 2027 (https://www.mountsinai.org/clinical-trials/devrobust-treatment-for-mal-de-d-barquement-syndrome).
References
Cohen B (2019) Dedication to Mingjia Dai, Ph.D. for Discovery of the First Successful Treatment of the Mal de Debarquement Syndrome. Front Neurol 10: 1196. doi: 10.3389/fneur.2019.01196
Cohen B, Yakushin SB, Cho C (2018) Hypothesis: The Vestibular and Cerebellar Basis of the Mal de Debarquement Syndrome. Front Neurol 9: 28. doi: 10.3389/fneur.2018.00028
Dai M, Cohen B, Cho C, Shin S, Yakushin SB (2017) Treatment of the Mal de Debarquement Syndrome: A 1-Year Follow-up. Front Neurol 8: 175. doi: 10.3389/fneur.2017.00175
Dai M, Cohen B, Smouha E, Cho C (2014) Readaptation of the vestibulo-ocular reflex relieves the mal de debarquement syndrome. Front Neurol 5: 124. doi: 10.3389/fneur.2014.00124
Dai MJ, Raphan T, Cohen B (1991) Spatial orientation of the vestibular system: dependence of optokinetic after-nystagmus on gravity. J Neurophysiol 66: 1422-39. doi: 10.1152/jn.1991.66.4.1422
Yakushin SB, Zink R, Clark BC, Liu C (2020) Readaptation Treatment of Mal de Debarquement Syndrome With a Virtual Reality App: A Pilot Study. Front Neurol 11: 814. doi: 10.3389/fneur.2020.00814
![]()