By Marcello Cherchi, MD PhD
For patients
When an airplane goes up, and when it comes down, you may experience pressure changes in your ears. Some doctors recommend using decongestants or ear plugs to help with this.
For clinicians
Practical summary
Airplane cabin pressure at cruising altitude is less than atmospheric pressure at sea level. During airplane ascent, ambient (cabin) pressure becomes less than middle ear pressure, and this pressure differential will cause the tympanic membrane to bulge outward. Properly functioning Eustachian tubes will eventually equalize this pressure. Then during airplane ascent, ambient (cabin) pressure becomes greater than middle ear pressure, and the pressure differential will cause the tympanic membrane to bulge inward. Again properly functioning Eustachian tubes will eventually equalize this pressure. However, in patients with Eustachian tube dysfunction, pressure equalization may not occur (or not be adequate), causing middle ear dysfunction, sometimes with corresponding audiologic and/or vestibular symptoms. Various management strategies have been studied, though none is very well supported by the evidence. The best (though still only moderate) evidence suggests that oral pseudoephedrine is superior to placebo. Evidence regarding the use of pressure-equalizing ear plugs is weak, but many patients elect this strategy because it incurs no medical risk.
Introduction
In commercial airplanes, at cruising altitude the cabin is pressurized to about 75% of sea-level atmospheric pressure (Mirza and Richardson 2005), approximately equivalent to the atmospheric pressure at an altitude of 1800 – 2400 meters above sea level (Mitchell-Innes et al. 2014). The change to this pressure during airplane ascent, and the change from this pressure during airplane descent, can cause pressure differentials between the middle ear and the ambient (airplane cabin) pressure. Mirza and Richardson explain the physiologic consequences of this as follows (Mirza and Richardson 2005):
Ascending
In a modern aircraft at cruising altitude, the cabin is pressurized to raise the air pressure to approximately three–quarters that of the ground atmospheric pressure. Therefore, as an aircraft ascends the atmospheric pressure decreases and the gas in the middle ear expands in accordance with Boyle’s law. If the eustachian tube is not opened by, for example, swallowing, then the middle ear gas, with a relatively positive pressure, will continue to expand until the tympanic membrane is pushed laterally to its limit, an effect which can be seen with an otoscope during flight. At a pressure differential of 15 mm Hg, the eustachian tube (if functioning properly) passively opens and vents off the positive pressure air, thereby equalizing the ambient and middle-ear pressures. This process of passive venting is rarely a problem on ascent and occurs at about every 122 m (400 ft) of increasing altitude. However, ear discomfort and pain can occur if there is eustachian tube dysfunction.
Descending
As an aircraft descends, the atmospheric pressure increases back to ‘normal’ and therefore the gas in the middle ear contracts, again in accordance with Boyle’s law. Now the eustachian tube behaves differently in descent as compared with ascent, in that air does not normally enter the middle ear passively and this is why aerotitis media tends to be more common and severe with descent. Muscular activity must open the auditory tube and this is usually achieved easily by swallowing or yawning. The tube can also be opened by some degree of overpressure applied at the nasal end, as in Valsalva’s manoeuvre. These manoeuvres become increasingly difficult if the pressure differential between the middle ear and atmosphere is allowed to increase during descent. At a pressure differential of 60 mmHg (i.e. the ambient pressure is 60 mmHg greater than the middle-ear pressure) fullness of the middle ear occurs and passengers experience discomfort. A pressure differential of around 80 mmHg closes the soft nasopharyngeal end of the tube with a force greater than that which can be developed by the muscles that open the tube. At this stage the tube will stay ‘locked’ and any attempts to equalize the pressure become futile. Beyond this point, the pathophysiological changes of barotrauma will occur. Performing Valsalva’s manoeuvre at this stage may become counter-productive by magnifying the already increasing overpressure in the nasopharynx. The pressure differential at which tube- locking occurs is variable, and will depend on the intrinsic strength of the tubal dilator muscles in any particular individual.
The corresponding anatomical changes in the tympanic membrane have been reported in 10% of adults (Mitchell-Innes et al. 2014; Stangerup et al. 1998; Wright 2015).
Treatments
Various strategies have been studied in the management of middle ear problems during airplane travel (Basu 2007; Wright 2015), including oral decongestants, nasal decongestants, ear plugs, myringotomy, and a variety of maneuvers that promote Eustachian tube patency (auto-insufflation, Valsalva, chewing, swallowing, yawning). Most passengers are unaware that such strategies are available (Mitchell-Innes et al. 2014).
A prospective placebo-controlled clinical trial comparing oral pseudoephedrine, nasal oxymetazoline and a double placebo (placebo pill and placebo nasal spray) found that pseudoephedrine was superior to placebo, while oxymetazoline was barely superior to placebo (Jones et al. 1998). Another prospective study reported oral pseudoephedrine to be superior to placebo (Csortan et al. 1994). A systematic review regarded these as providing moderate evidence in support of using oral pseudoephedrine.
Pressure-equalizing earplugs have been studied (Berger 2006). One trial comparing pressure-equalizing ear plugs with placebo (ear plugs without pressure equalization properties) reported no difference (Klokker et al. 2005). In contrast, another study reported subjective improvement in ear symptoms (Jumah et al. 2010). A systematic review concluded that there is insufficient evidence to recommend pressure-equalizing ear plugs (Ryan et al. 2018). However, since such ear plugs are relatively inexpensive and incur no medical risk, many patients choose this strategy (as opposed to taking medications). The Figure below shows examples of pressure-equalizing earplugs.
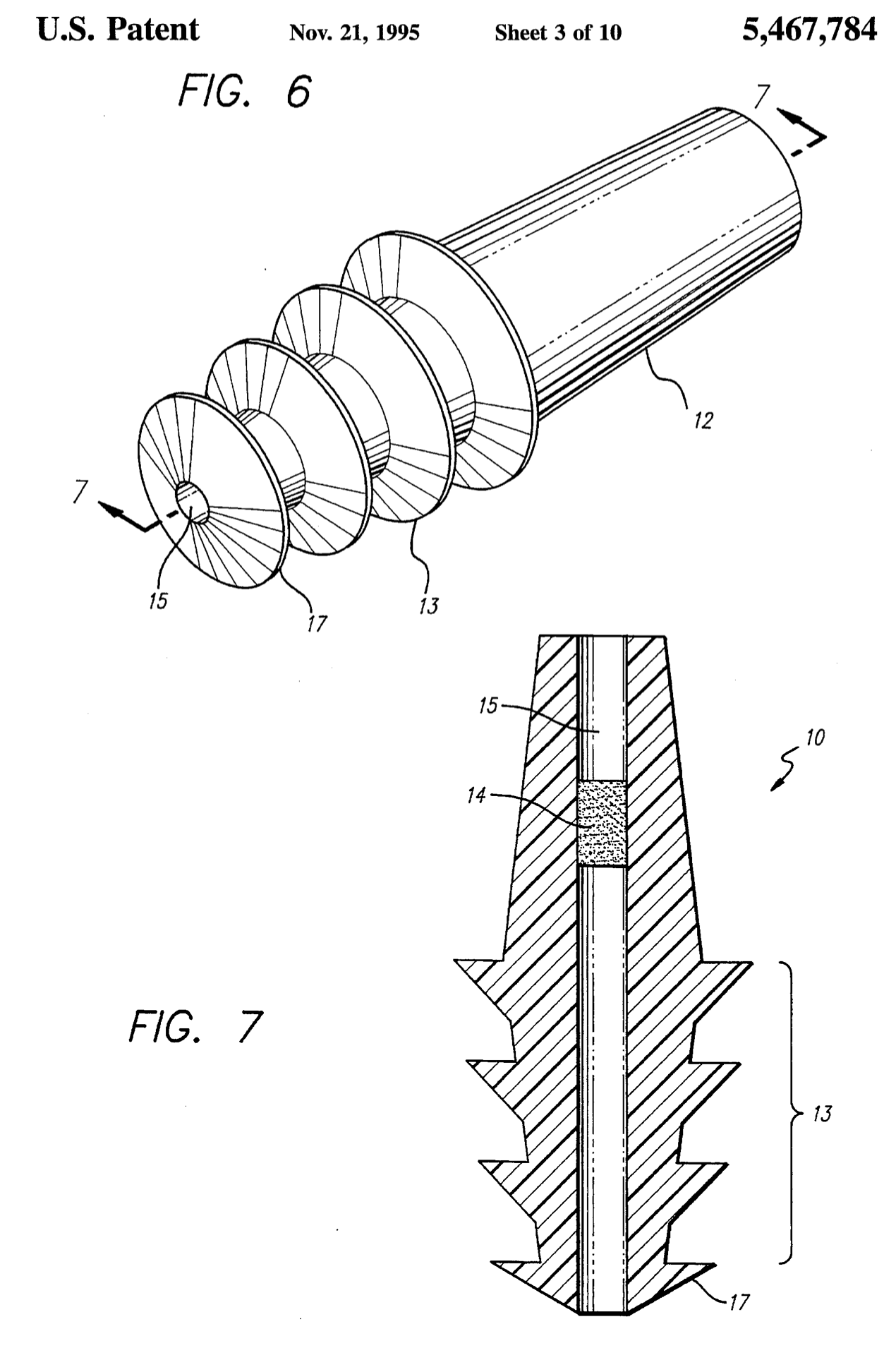
Source: https://patentcenter.uspto.gov/applications/08291165
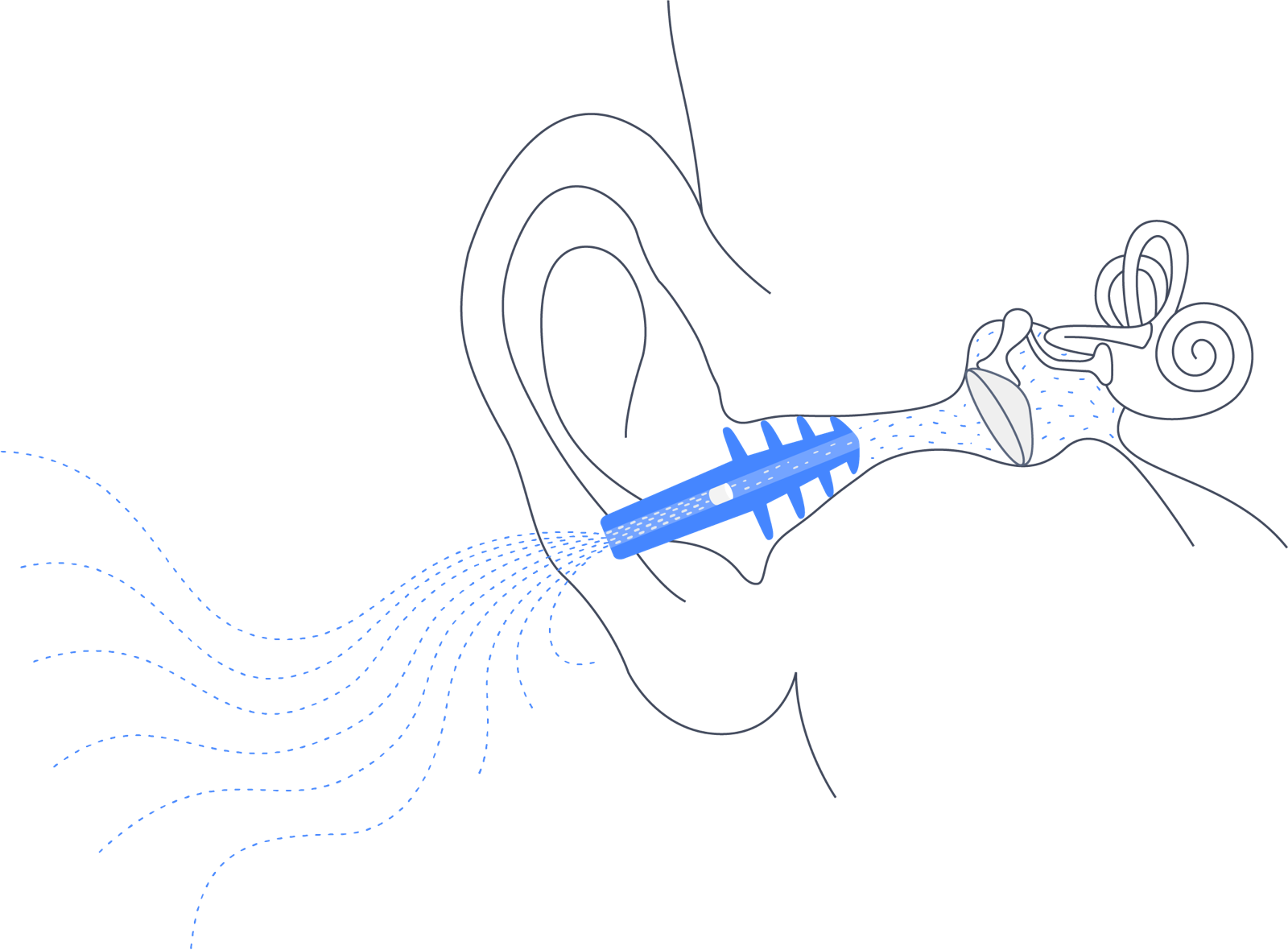
Source: https://www.earplanes.com
Adverse effects
Pseudoephedrine is a sympathomimetic, with the correspondingly predictable adverse effects of a stimulant.
Cautions and contraindications
Ear plugs are relatively contraindicated in patients with ear injuries, active ear infections, or copious cerumen.
Pseudoephedrine is relatively contraindicated in patients on certain other medications (such as monoamine oxidase inhibitors, alpha and beta adrenergic agonists) and certain medical conditions (pregnancy, cardiovascular disease, glaucoma, hyperthyroidism).
Relevance in otoneurology
Changes in middle ear pressure can provoke audiologic and vestibular symptoms in diseases such as semicircular canal dehiscence and perilymphatic fistula.
One would think that such pressure changes might also increase the risk of benign paroxysmal positional vertigo (BPPV), and anecdotally many patients report exacerbations of BPPV following airplane travel, but as of this writing no clear evidence had been published in support of this idea.
Other notes
In the United States there has been concern about pseudoephedrine being misused in clandestine labs to synthesize methamphetamine. As of this writing, pseudoephedrine remains available without a prescription (“over-the-counter”) in most states. Other states have passed laws requiring that this drug be maintained in locked pharmacy storage (“behind-the-counter”), and that there be monthly dispensing limits per individual, though it is still available without a prescription (Shi and Ganiats 2007). Some states have reclassified pseudoephedrine as a schedule III substance, requiring a prescription (Cunningham et al. 2012).
References
Basu A (2007) Middle ear pain and trauma during air travel. BMJ Clin Evid 2007.
Berger EH (2006) Pressure-equalizing earplugs. Aviat Space Environ Med 77: 766; author reply 766.
Csortan E, Jones J, Haan M, Brown M (1994) Efficacy of pseudoephedrine for the prevention of barotrauma during air travel. Ann Emerg Med 23: 1324-7. doi: 10.1016/s0196-0644(94)70359-0
Cunningham JK, Callaghan RC, Tong D, Liu LM, Li HY, Lattyak WJ (2012) Changing over-the-counter ephedrine and pseudoephedrine products to prescription only: impacts on methamphetamine clandestine laboratory seizures. Drug Alcohol Depend 126: 55-64. doi: 10.1016/j.drugalcdep.2012.04.011
Jones JS, Sheffield W, White LJ, Bloom MA (1998) A double-blind comparison between oral pseudoephedrine and topical oxymetazoline in the prevention of barotrauma during air travel. Am J Emerg Med 16: 262-4. doi: 10.1016/s0735-6757(98)90097-3
Jumah MD, Schlachta M, Hoelzl M, Werner A, Sedlmaier B (2010) Pressure regulating ear plug testing in a pressure chamber. Aviat Space Environ Med 81: 560-5. doi: 10.3357/asem.2717.2010
Klokker M, Vesterhauge S, Jansen EC (2005) Pressure-equalizing earplugs do not prevent barotrauma on descent from 8000 ft cabin altitude. Aviat Space Environ Med 76: 1079-82.
Mirza S, Richardson H (2005) Otic barotrauma from air travel. J Laryngol Otol 119: 366-70. doi: 10.1258/0022215053945723
Mitchell-Innes A, Young E, Vasiljevic A, Rashid M (2014) Air travellers’ awareness of the preventability of otic barotrauma. J Laryngol Otol 128: 494-8. doi: 10.1017/S0022215114001145
Ryan P, Treble A, Patel N, Jufas N (2018) Prevention of Otic Barotrauma in Aviation: A Systematic Review. Otol Neurotol 39: 539-549. doi: 10.1097/MAO.0000000000001779
Shi CW, Ganiats TG (2007) Perceptions about behind-the-counter availability of pseudoephedrine. Am J Health Syst Pharm 64: 236-7. doi: 10.2146/ajhp060541
Stangerup SE, Tjernström O, Klokker M, Harcourt J, Stokholm J (1998) Point prevalence of barotitis in children and adults after flight, and effect of autoinflation. Aviat Space Environ Med 69: 45-9.
Wright T (2015) Middle-ear pain and trauma during air travel. BMJ Clin Evid 2015.
![]()