By Marcello Cherchi, MD PhD
For patients
The middle ear (the space immediately behind the eardrum) can become inflamed, or filled with fluid, or infected. Symptoms can include ear discomfort, hearing loss or disequilibrium. Your doctor may examine you by looking in your ear with a microscope or otoscope. In some cases, tests of hearing or balance function may be appropriate. If the cause is thought to be infectious, your doctor may prescribe a course of antibiotics. If that fails, then you may be referred to an otolaryngologist.
For clinicians
Overview
The middle ear space can be filled with a (non-inflammatory, non-infectious) effusion; it can be affected by inflammation (with or without effusion) or infection. Typical symptoms include aural fullness and pain, and possibly hearing loss and disequilibrium. This condition is more frequent in children, probably because of the orientation of the Eustachian tube. Physical examination under otomicroscopy or otoscopy may show a fluid meniscus behind the tympanic membrane; in some cases there may be nystagmus, though the patterns of nystagmus are neither specific nor sensitive for these middle ear conditions. The hearing loss, if assessed by audiometry, is usually conductive in nature. Some cases may have detectable abnormalities on otovestibular testing (vestibular evoked myogenic potentials, video head impulse testing, ocular motor testing, caloric testing, rotatory chair testing, posturography). Imaging is usually not necessary with an initial episode. If there is reason to suspect infection, then empiric treatment with antibiotics is reasonable. If that fails, then referral to otolaryngology is appropriate to be evaluated for myringotomy or placement of a grommet.
Terminology
The phrase “middle ear effusion” refers to fluid in the middle ear. If the fluid is neither inflammatory nor infectious, then it is usually referred to as a “serous middle ear effusion.”
The phrase “otitis media” refers to an inflammatory process in the middle ear space, irrespective of whether any effusion is also present. If fluid is also present but no infection is involved, then it is referred to as “serous otitis media.” If otitis media involves infection, then it is designated according to the pathogen (e.g., “bacterial otitis media,” “tuberculous otitis media,” etc.”).
Epidemiology
Middle ear effusion and inflammation are more common in children than in adults, though some studies have also been conducted on adults (Mostafa, Shafik et al. 2013, Kalaycik Ertugay, Kulekci et al. 2015, Aarhus, Tambs et al. 2016, Kim, Lee et al. 2021, Tailor, Phillips et al. 2022).
Risk factors for middle ear effusion and inflammation include Eustachian tube dysfunction.
Pathophysiology
Effusion, inflammation or infection in the middle ear space have the potential to provoke aural symptoms (pain, fullness), auditory symptoms (hearing loss, tinnitus) and vestibular symptoms (disequilibrium).
Presentation: Hearing loss
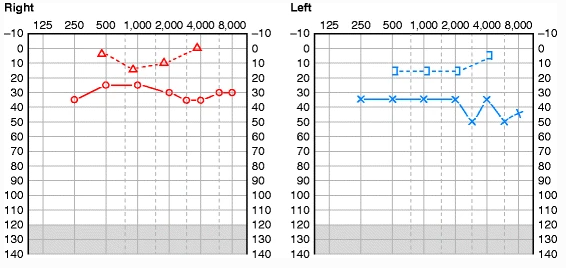
Hearing loss is fairly common in cases of otitis media (Leskinen 2005, Hyden, Akerlind et al. 2006, Kalaycik Ertugay, Kulekci et al. 2015, Kim, Yang et al. 2016, Kim, Lee et al. 2021). The associated hearing loss is usually conductive, and is due to mechanical interference with the motion of the ossicular chain.
The Figure below, from Zaidi and Sinha (Zaidi and Sinha 2013), shows bilateral conductive hearing loss in a case of chronic bilateral suppurative otitis media.
Presentation: Disequilibrium
Vestibular symptoms are less common than auditory ones in middle ear effusions and otitis media, but do occur (Grace and Pfleiderer 1990, Leskinen 2005, Hyden, Akerlind et al. 2006, Gianoli and Soileau 2008, Kalaycik Ertugay, Kulekci et al. 2015, Saliba, Dagher et al. 2015, Aarhus, Tambs et al. 2016, Kim, Yang et al. 2016, Monsanto, Kasemodel et al. 2018, Monsanto, Kasemodel et al. 2020, Kim, Lee et al. 2021, Tailor, Phillips et al. 2022).
It is certainly possible for otitis media to develop into labyrinthitis (Hyden, Akerlind et al. 2006, Kitsko and Dohar 2007, Zaidi and Sinha 2013, Kim, Yang et al. 2016, Choi, Han et al. 2019). In such cases, presumably pathogens pass from the middle ear to the inner ear by traversing the oval and/or round windows. Labyrinthitis has been well-studied, and it is unsurprising that such patients can have vestibular symptoms.
But there are other cases of middle ear effusions and otitis media that do not appear to evolve into labyrinthitis, yet are still associated with vestibular symptoms. In such cases, the mechanism by which the middle ear process provokes vestibular symptoms is unclear. Temporal bone studies of patients who in life had chronic otitis media show reduced density of type I and type II vestibular hair cells and of dark cells (da Costa Monsanto, Erdil et al. 2016), suggesting that even if these patients do not clinically present with a discrete episode suggestive of labyrinthitis, the chronic otitis media still provokes pathology in the labyrinth.
Physical examination: Otomicroscopy/otoscopy
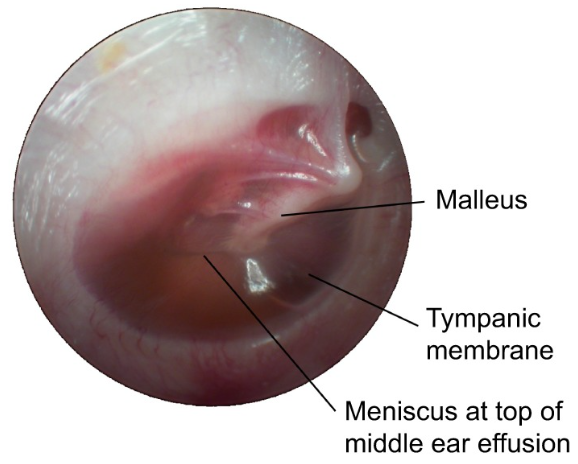
A binocular otomicroscopic examination, or at least a monocular otoscopic examination, is important in these patients. A middle ear effusion is often (though not always) visible as a fluid meniscus behind the tympanic membrane.
The Figure below, from Bhutta and colleagues (Bhutta, Thornton et al. 2017), shows a fluid meniscus from a serous middle ear effusion.
Physical examination: Nystagmus
Some investigators report nystagmus of various patterns in cases of acute otitis media (Kim, Yang et al. 2016, Choi, Han et al. 2019, Kim, Lee et al. 2021), including direction changing positional nystagmus, and direction-fixed nystagmus (paretic or irritative). One series of patients with acute otitis media without vestibular complaints reported nystagmus in 82% (28 out of 34) of patients; we find this statistic impressive, and far greater than in our own experience.
Testing
Audiometry often shows hearing loss (usually conductive) in the affected ear (Eliashar, Gross et al. 2004, Zaidi and Sinha 2013, Tailor, Phillips et al. 2022). Tympanometry often shows reduced compliance (peak immittance).
Vestibular evoked myogenic potentials are sometimes abnormal (Mostafa, Shafik et al. 2013) in a middle ear with effusion or inflammation, but whether this is an artifact of conductive hearing loss or reflects true vestibular dysfunction is not always clear. In this regard, some studies are careful to compare air-conducted and bone-conducted vestibular evoked myogenic potentials (Kolkaila, Emara et al. 2015).
Some patients with middle ear effusion or inflammation exhibit abnormalities on video head impulse testing, usually in the form of the presence of corrective saccades, or reduced gain (Abdelmotaleb, Sobhy et al. 2023). Comert and colleagues (Comert, Sencan et al. 2021) more specifically observed covert compensatory saccades in 32% of the patients, and reduced gain in the anterior canal on the affected side.
Several studies have explored ocular motor function with electronystagmography or videonystagmography in patients with middle ear effusion and/or inflammation. Eliashar and colleagues reported an “abnormal electronystagmogram” in all patients who had vestibular complaints; these “abnormalities” included spontaneous nystagmus and direction changing nystagmus. Gianoli and colleagues reported unilateral or bilateral caloric weakness in 19 (76%) out of 25 patients with chronic suppurative otitis media (Gianoli and Soileau 2008). Golz and colleagues (Golz, Netzer et al. 1998) studied 136 patients with middle ear effusion and reported abnormal electronystagmographic findings in 58% of patients, including 42 (31%) who exhibited spontaneous unidirectional nystagmus, and 24 (17.5%) who exhibited positional nystagmus. Lee and colleagues (Lee, Park et al. 2009) studied 25 patients with unilateral chronic otitis media and reported that 20 (80%) showed some ocular motor abnormality, with 5 (20%) exhibiting unilateral caloric weakness, 12 (48%) exhibiting head shaking nystagmus, and 7 (28%) exhibiting vibration induced nystagmus. Mostafa and colleagues (Mostafa, Shafik et al. 2013) studied 58 adults (mean age 29.5 years) and found 62% had a caloric weakness. Saliba and colleagues (Saliba, Dagher et al. 2015) studied 15 children with chronic middle ear effusion and found 2 (13%) had abnormal ocular motor findings, 1 with positional nystagmus, and 1 with both spontaneous and positional nystagmus.
Mostafa and colleagues (Mostafa, Shafik et al. 2013) studied 58 adults (mean age 29.5 years) and found 70% of patients rotatory chair abnormalities.
Of other vestibular tests, Lee and colleagues (Lee, Park et al. 2009) studied 25 patients with unilateral chronic otitis media and reported that 5 (20%) had abnormal subjective visual vertical (suggesting otolith dysfunction).
Some studies report abnormal findings on static or dynamic posturography (Gawron, Pospiech et al. 2004, Monsanto, Kasemodel et al. 2020, Abdelmotaleb, Sobhy et al. 2023).
Interestingly, of patients with abnormal vestibular test findings, not all complain of disequilibrium. For example, Lee and colleagues (Lee, Park et al. 2009) studied 25 patients with unilateral chronic otitis media and reported that 20 (80%) showed some ocular motor abnormality, yet none of these patients complained of dizziness or vertigo. Kim and colleagues (Kim, Lee et al. 2021) used “video Frenzel glasses” to study 34 adult patients with acute otitis media and reported that 28 (82%) exhibited either direction changing positional nystagmus, direction-fixed irritative nystagmus or direction-fixed paretic nystagmus, yet none of these patients complained of dizziness or vertigo. These findings suggest that middle ear effusion and inflammation can cause sub-clinical vestibular deficits.
Imaging
Imaging is usually not warranted with an initial presentation of middle ear effusion/inflammation/infection. In a patient with recurrent bouts, imaging may be appropriate, though at that point the patient should probably have already been referred to otolaryngology. Otolaryngologists in that circumstance may consider an MRI of the skull base without and with contrast to evaluate for obstructive causes of Eustachian tube dysfunction, mastoiditis or an abscess.
Treatment: Medical
Many cases of middle ear effusion resolve spontaneously.
If a middle ear effusion develops a superimposed infection, then antibiotic therapy is appropriate. In a patient without penicillin allergy, a course of amoxicillin, or amoxicillin-clavulanate is reasonable. In a patient with a penicillin allergy, consider a course of cefdinir, cefuroxime or cefpodoxime. If those approaches fail, then (whether or not the patient has a penicillin allergy), consider a course of ceftriaxone. If antibiotic treatment is failing, then the clinician should have a low threshold for referral to otolaryngology.
Treatment: Surgical
For patients with infectious otitis media who have failed empiric courses of antibiotics, referral to otolaryngology is appropriate. Commonly attempted procedures in this circumstance include myringotomy (Kim, Yang et al. 2016) or placement of a grommet (Grace and Pfleiderer 1990, Golz, Westerman et al. 1991, Golz, Netzer et al. 1998). These case series report significant improvement in auditory and vestibular symptoms.
References
Aarhus L, Tambs K, Hoffman HJ, Engdahl B (2016) Childhood otitis media is associated with dizziness in adulthood: the HUNT cohort study. Eur Arch Otorhinolaryngol 273: 2047-54. doi: 10.1007/s00405-015-3764-9
Abdelmotaleb H, Sobhy O, Bassiouny M, Elsherif M (2023) Evaluation of postural stability and vestibulo-ocular reflex in adults with chronic suppurative otitis media. Eur Arch Otorhinolaryngol 280: 897-905. doi: 10.1007/s00405-022-07687-y
Bhutta MF, Thornton RB, Kirkham LS, Kerschner JE, Cheeseman MT (2017) Understanding the aetiology and resolution of chronic otitis media from animal and human studies. Dis Model Mech 10: 1289-1300. doi: 10.1242/dmm.029983
Choi JW, Han K, Nahm H, Shin JE, Kim CH (2019) Direction-Changing Positional Nystagmus in Acute Otitis Media Complicated by Serous Labyrinthitis: New Insights into Positional Nystagmus. Otol Neurotol 40: e393-e398. doi: 10.1097/MAO.0000000000002104
Comert E, Sencan Z, Kocak FM, Simsek G, Muluk NB (2021) Clinical evaluation of the vestibular impairment using video head impulse test In children with acute otitis media. Int J Pediatr Otorhinolaryngol 141: 110568. doi: 10.1016/j.ijporl.2020.110568
da Costa Monsanto R, Erdil M, Pauna HF, Kwon G, Schachern PA, Tsuprun V, Paparella MM, Cureoglu S (2016) Pathologic Changes of the Peripheral Vestibular System Secondary to Chronic Otitis Media. Otolaryngol Head Neck Surg 155: 494-500. doi: 10.1177/0194599816646359
Eliashar R, Gross M, Saah D, Elidan J (2004) Vestibular involvement in myringitis bullosa. Acta Otolaryngol 124: 249-52. doi: 10.1080/00016480310015308
Gawron W, Pospiech L, Orendorz-Fraczkowska K (2004) An evaluation of postural stability and the effects of middle-ear drainage on vestibulo-spinal reflexes of children with chronic otitis media with effusion. Int J Pediatr Otorhinolaryngol 68: 1175-9. doi: 10.1016/j.ijporl.2004.03.017
Gianoli GJ, Soileau JS (2008) Chronic suppurative otitis media, caloric testing, and rotational chair testing. Otol Neurotol 29: 13-5. doi: 10.1097/mao.0b013e31815c2589
Golz A, Netzer A, Angel-Yeger B, Westerman ST, Gilbert LM, Joachims HZ (1998) Effects of middle ear effusion on the vestibular system in children. Otolaryngol Head Neck Surg 119: 695-9. doi: 10.1016/S0194-5998(98)70039-7
Golz A, Westerman ST, Gilbert LM, Joachims HZ, Netzer A (1991) Effect of middle ear effusion on the vestibular labyrinth. J Laryngol Otol 105: 987-9. doi: 10.1017/s002221510011802x
Grace AR, Pfleiderer AG (1990) Dysequilibrium and otitis media with effusion: what is the association? J Laryngol Otol 104: 682-4. doi: 10.1017/s0022215100113611
Hyden D, Akerlind B, Peebo M (2006) Inner ear and facial nerve complications of acute otitis media with focus on bacteriology and virology. Acta Otolaryngol 126: 460-6. doi: 10.1080/00016480500401043
Kalaycik Ertugay C, Kulekci S, Naiboglu B, Ertugay OC, Kaya KS, Sheidaei S, Oysu C (2015) Clinical evaluation of inner ear changes as result of chronic otitis media and its surgery. Kulak Burun Bogaz Ihtis Derg 25: 22-7. doi: 10.5606/kbbihtisas.2015.36048
Kim CH, Lee J, Choi B, Shin JE (2021) Nystagmus in adult patients with acute otitis media or otitis media with effusion without dizziness. PLoS One 16: e0250357. doi: 10.1371/journal.pone.0250357
Kim CH, Yang YS, Im D, Shin JE (2016) Nystagmus in patients with unilateral acute otitis media complicated by serous labyrinthitis. Acta Otolaryngol 136: 559-63. doi: 10.3109/00016489.2015.1132845
Kitsko DJ, Dohar JE (2007) Inner ear and facial nerve complications of acute otitis media, including vertigo. Curr Allergy Asthma Rep 7: 444-50. doi: 10.1007/s11882-007-0068-1
Kolkaila EA, Emara AA, Gabr TA (2015) Vestibular evaluation in children with otitis media with effusion. J Laryngol Otol 129: 326-36. doi: 10.1017/S0022215115000535
Lee IS, Park HJ, Shin JE, Jeong YS, Kwak HB, Lee YJ (2009) Results of air caloric and other vestibular tests in patients with chronic otitis media. Clin Exp Otorhinolaryngol 2: 145-50. doi: 10.3342/ceo.2009.2.3.145
Leskinen K (2005) Complications of acute otitis media in children. Curr Allergy Asthma Rep 5: 308-12. doi: 10.1007/s11882-005-0071-3
Monsanto RDC, Kasemodel ALP, Tomaz A, Elias TGA, Paparella MM, Penido NO (2020) Evaluation of vestibular symptoms and postural balance control in patients with chronic otitis media. J Vestib Res 30: 35-45. doi: 10.3233/VES-200691
Monsanto RDC, Kasemodel ALP, Tomaz A, Paparella MM, Penido NO (2018) Current evidence of peripheral vestibular symptoms secondary to otitis media. Ann Med 50: 391-401. doi: 10.1080/07853890.2018.1470665
Mostafa BE, Shafik AG, El Makhzangy AM, Taha H, Abdel Mageed HM (2013) Evaluation of vestibular function in patients with chronic suppurative otitis media. ORL J Otorhinolaryngol Relat Spec 75: 357-60. doi: 10.1159/000357475
Saliba I, Dagher C, El-Zir E, Yammine FG (2015) A Pilot Study to Assess the Vestibular Apparatus Function with Videonystagmography During Chronic Otitis Media with Effusion. Curr Pediatr Rev 11: 135-40. doi: 10.2174/1573396311666150702105027
Tailor BV, Phillips JS, Nunney I, Yung MW, Doruk C, Kara H, Kong T, Quaranta N, Penaranda A, Bernardeschi D, Dai C, Kania R, Denoyelle F, Tono T (2022) Presentation of dizziness in individuals with chronic otitis media: data from the multinational collaborative COMQ-12 study. Eur Arch Otorhinolaryngol 279: 2857-2863. doi: 10.1007/s00405-021-06993-1
Zaidi SH, Sinha A (2013) Chronic Suppurative Otitis Media (CSOM). In: Zaidi SH, Sinha A (eds) Vertigo: A Clinical Guide. Springer Berlin Heidelberg, Berlin, Heidelberg, pp 113-118
![]()