By Marcello Cherchi, MD PhD
For patients
Ramsay Hunt syndrome (RHS) is thought to be infection by the Varicella zoster virus that involves nerves responsible for hearing, balance, ear sensations and facial movements. Symptoms start abruptly, and may consist of disequilibrium, and one-sided ear symptoms of pain, hearing loss and tinnitus. Your physician may consider checking tests of hearing and balance, and may consider checking an MRI of the brain and internal auditory canals. There are no good treatments, though some advocate treatment with steroids and/or anti-viral agents. Symptoms are often severe and recovery is often poor.
For clinicians
Overview
Ramsay Hunt syndrome (RHS) is a cranial neuropathy mostly of the vestibulocochlear and facial nerves attributed to Varicella zoster virus infection. It can occur at any age (though is more common with increasing age), without clear gender predisposition. Presenting symptoms are some combination of facial weakness, aural pain, hearing loss, hyperacusis, tinnitus, disequilibrium and dysgeusia. Physical examination may show lower motor neuron facial weakness, sensorineural hearing loss, often a vesicular rash in the external auditory canal, less commonly nystagmus. Audiometry may show hearing loss, which tends to be more pronounced in the high frequencies. Vestibular testing (caloric testing, vestibular evoked myogenic potentials, video head impulse testing) may show evidence of unilateral vestibular hypofunction. MRI of the internal auditory canals without and with contrast may show enhancement of the vestibulocochlear and/or facial nerves. Treatment with steroids (prednisone, methylprednisolone) and anti-viral agents (usually valacyclovir) is often attempted, but data supporting efficacy are weak. Prognosis is guarded; the facial weakness is more severe and recovers more poorly than in Bell’s palsy; the hearing may recover more poorly than in labyrinthitis; the disequilibrium may recover more poorly than in vestibular neuritis. A patient in whom Ramsay Hunt syndrome is suspected or diagnosed is often referred to an otoneurologist or neuro-otologist.
Introduction
In 1907 the American neurologist, James Ramsay Hunt (1872 – 1937), published a paper describing varicella zoster affectation of the vestibulocochlear nerve and facial nerve (Hunt 1907).

This clinical entity is sometimes designated Herpes zoster oticus, but that nomenclature implies that only the vestibulocochlear nerve is affected. In fact, patients usually present with some combination of affectation of the vestibulocochlear and facial nerves.
Epidemiology
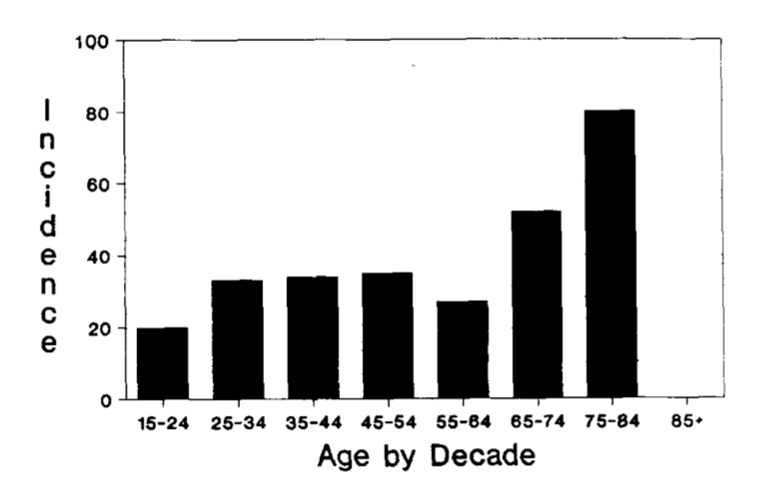
The incidence of Ramsay Hunt syndrome increases with age, though it can still affect pediatric patients (Hato, Kisaki et al. 2000, Kansu and Yilmaz 2012). The Chart below, from Wayman and colleagues (Wayman, Pham et al. 1990), is a histogram showing the age distribution by decade.
Literature reports conflicting data regarding gender predominance of disease distribution.
Some studies report a slight female preponderance. The series of 186 Ramsay Hunt patients studied by Wayman and colleagues (Wayman, Pham et al. 1990) included 102 (55%) females and 85 (45%) males. The series of 185 Ramsay Hunt patients studied by Robillard and colleagues (Robillard, Hilsinger et al. 1986) reported 101 (54.6%) females and 84 (45.4%) males.
In contrast, other studies report a male preponderance. In the series of 13 Ramsay Hunt patients studied by Martin-Sanz and colleagues (Martin-Sanz, Rueda et al. 2017), 7 (54%) were male and 6 (46%) were female; since these statistics are almost exactly the opposite of the others, we conclude that it is an artifact of the small sample size (13 patients, rather than 185 and 186 patients in the previously cited 2 studies). However, an investigation with a larger sample size, Coulson and colleagues (Coulson, Croxson et al. 2011) studied 101 patients with Ramsay Hunt syndrome, and the study population comprised 70 (70%) males and 31 (31%) females.
Clinical presentation
Patients present with some combination of:
- Vestibulocochlear symptoms (disequilibrium, hearing loss, tinnitus). These are believed to result from direct affectation of the vestibulocochlear nerve by the Varicella zoster virus (VZV).
- Ipsilateral facial weakness. Edema of the vestibulocochlear nerve within the internal auditory canal may compress the facial nerve and cause paresis. Another possibility is passage of infection from the vestibulocochlear nerve to the facial nerve (Kuhweide, Van de Steene et al. 2002). Since most of the facial nerve supplies facial muscles, the VZV eruptions do not occur on the face (whose sensory innervation would be supplied by the trigeminal nerve).
- Vesicular lesions in the ipsilateral internal auditory canal. This may be compatible with VZV involvement of the nervus intermedius — somatosensory fibers that run within the facial nerve to supply “parts of both the medial and lateral surfaces of the auricle, to a strip along the external acoustic meatus, and to a part of the tympanic cavity” (Rhoton, Kobayashi et al. 1968) — or possibly somatosensory fibers within the vestibulocochlear nerve.
The multiple symptoms may present approximately simultaneously, or serially but in fairly close temporal proximity (Iwasaki, Toda et al. 2013).
In a series of 14 patients with Ramsay Hunt syndrome, Iwasaki and colleagues (Iwasaki, Toda et al. 2013) reported that 14 (100%) had lower motor neuron facial weakness (House-Brackman grade IV – VI), 12 (86%) had disequilibrium, and 10 (71%) had hearing loss ipsilateral to the facial palsy.
In the series of Ramsay Hunt patients studied by Wayman and colleagues (Wayman, Pham et al. 1990), of 93 patients with normal audiometry only 5 (5%) complained of disequilibrium, and of 29 patients with abnormal audiometry 8 (28%) complained of disequilibrium.
Despite the hearing loss, some patients also complain of hyperacusis. Two potential contributors to this include loudness recruitment, and malfunction of the stapedius (mediated by the nerve to the stapedius, which is from the facial nerve that is paretic in Ramsay Hunt syndrome).
In the series of Ramsay Hunt patients studied by Wayman and colleagues (Wayman, Pham et al. 1990), of 93 with normal audiograms, 44 (47%) reported hyperacusis, and 45 (48%) reported hearing loss and tinnitus; of 29 with abnormal audiograms, 5 (31%) reported hyperacusis and 5 (31%) reported hearing loss and tinnitus.
Some patients also complain of dysgeusia (Robillard, Hilsinger et al. 1986, Adour 1994), presumably due to affectation of the afferents passing through the chorda tympani (gustatory branch of the facial nerve).
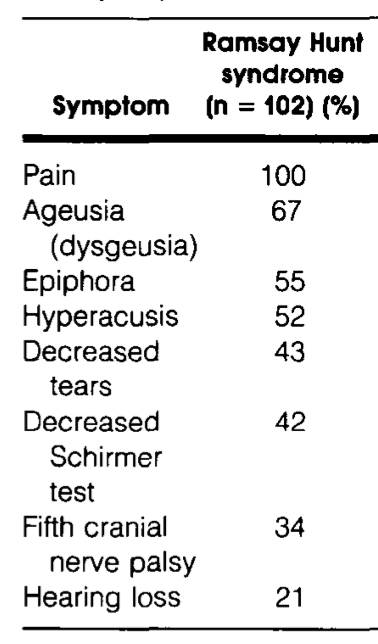
Robillard and colleagues (Robillard, Hilsinger et al. 1986) reported facial, aural and auditory symptoms (not disequilibrium) in a series of 102 Ramsay Hunt syndrome patients, as shown in the Table below. Notable points include that 100% experienced pain, 67% experienced disturbances of taste, 52% experienced hyperacusis and 21% experienced hearing loss.
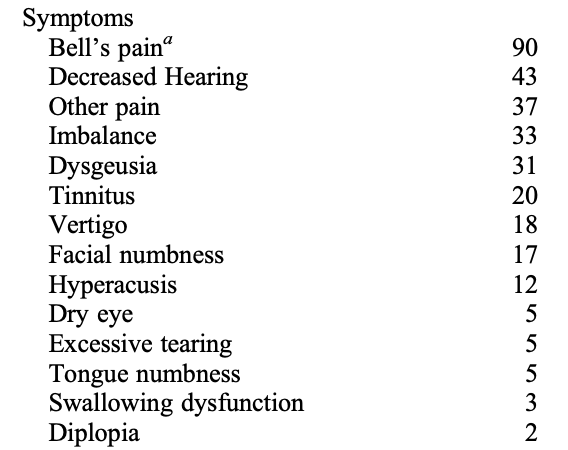
Coulson and colleagues (Coulson, Croxson et al. 2011) studied findings in 101 patients with Ramsay Hunt syndrome, and reported the findings in the Table below; the numbers listed are percentages. Notable points include that 90% of patients complained of ear pain, 43% of hearing loss, 33% of disequilibrium, 31% of gustatory abnormalities, 20% of tinnitus and 12% of hyperacusis.
The Table below compares data regarding symptoms from the studies discussed earlier.
|
Symptom |
Robillard et al. (Robillard, Hilsinger et al. 1986) |
Coulson et al. (Coulson, Croxson et al. 2011) |
Iwasaki et al. (Iwasaki, Toda et al. 2013) |
Wayman et al. (Wayman, Pham et al. 1990), patients with normal audiometry |
Wayman et al. (Wayman, Pham et al. 1990), patients with abnormal audiometry |
|
Facial weakness |
— |
— |
100% |
— |
|
|
Aural pain |
100% |
90% |
43% |
72% |
|
|
Hearing loss |
21% |
43% |
71% |
48% |
31% |
|
Hyperacusis |
52% |
12% |
— |
47% |
31% |
|
Tinnitus |
20% |
— |
— |
48% |
|
|
Disequilibrium |
— |
33% (“imbalance”) 18% (“vertigo”) |
86% |
5% |
28% |
|
Dysgeusia |
67% |
31% |
— |
— |
— |
Table : Comparison of data from multiple studies regarding symptoms in Ramsay Hunt syndrome.
Physical examination
A minority of patients lack the vesicular lesions (Adour 1994), which parallels the “herpete sine herpete” dermatological manifestations of Varicella zoster affecting other areas of the body. In the study by Coulson and colleagues (Coulson, Croxson et al. 2011) of 101 patients with Ramsay Hunt syndrome, 75% presented with vesicular lesions — in other words, 25% of patients lack the vesicular lesions. In the study by Wayman and colleagues (Wayman, Pham et al. 1990) of 132 patients with Ramsay Hunt syndrome, 122 had audiometry performed; of those 122 patients, 37/93 (40%) with normal hearing had vesicular lesions, and 18/29 (62%) with abnormal hearing had vesicular lesions.
In the study by Coulson and colleagues (Coulson, Croxson et al. 2011) of 101 patients with Ramsay Hunt syndrome, 5% presented with “nystagmus.”
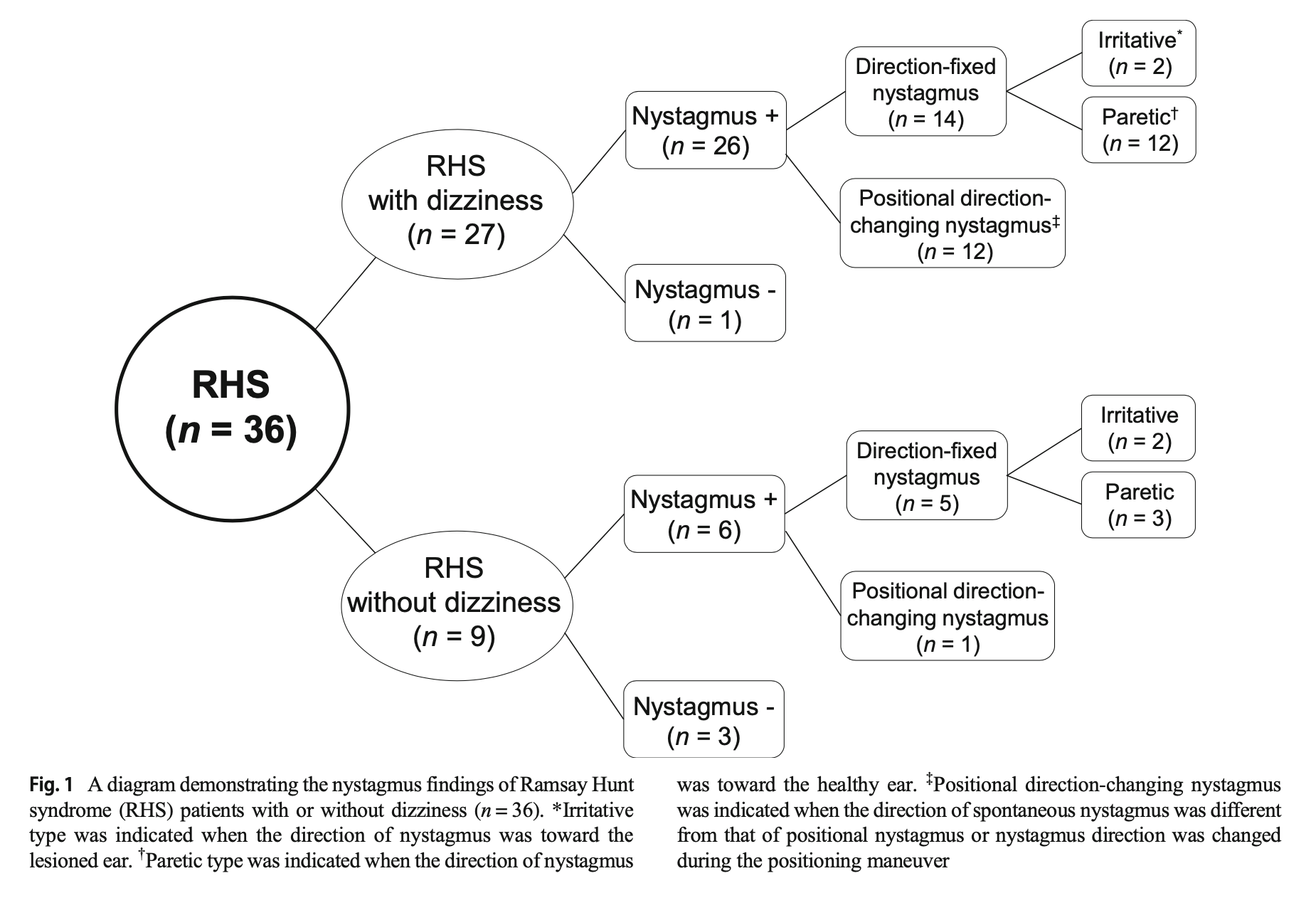
Lee and colleagues (Lee, Choi et al. 2021) studied 36 patients with Ramsay Hunt syndrome; of 27 patients who complained of disequilibrium, 26 (96%) exhibited nystagmus, and of 9 patients who did not complain of disequilibrium, 6 (67%) still showed nystagmus. In these patients they identified direction-fixed nystagmus (either irritative or paretic) and direction-changing positional nystagmus. The Figure below summarizes their findings.
Kim and colleagues (Kim, Choi et al. 2018) studied 28 patients with Ramsay Hunt syndrome who complained of disequilibrium. The patterns of nystagmus they reported were: 61% direction-fixed nystagmus that was contraversive (beating away from the lesion); 18% direction-changing positional nystagmus that was apogeotropic; 14% direction-fixed nystagmus that was ipsiversive (beating away from the lesion); and 7% direction-changing positional nystagmus that was apogeotropic.
Testing: audiometry
In a series of 14 patients with Ramsay Hunt syndrome, Iwasaki and colleagues (Iwasaki, Toda et al. 2013) reported that audiometry showed sensorineural hearing loss in 10 (71%) ipsilateral to the facial palsy.
In a series of 152 patients with Ramsay Hunt syndrome who had audiometry performed, Wayman and colleagues (Wayman, Pham et al. 1990) noted that 93 (61%) showed normal hearing, and 29 (19%) showed hearing loss attributed to Ramsay Hunt syndrome; the remaining 30 (20%) were deemed to have hearing loss from other causes.
The hearing loss tends to be more severe in the high frequencies. Hearing loss tends to be more severe in patients with disequilibrium. The degree of hearing loss does not correlate significantly with the facial weakness (Kim, Choi et al. 2016).
Testing: vestibular assessment with caloric testing
In a series of 19 patients with Ramsay Hunt syndrome, Takahashi and colleagues (Takahashi, Sato et al. 2021) reported that 15 (79%) exhibited caloric weakness.
In a series of 14 patients with Ramsay Hunt syndrome, Iwasaki and colleagues (Iwasaki, Toda et al. 2013) reported that 12 (86%) had caloric weakness ipsilateral to the facial palsy — the same 12 patients who complained of disequilibrium.
In a series of 10 patients with Ramsay Hunt syndrome, Ozeki and colleagues (Ozeki, Iwasaki et al. 2006) reported that 10 (100%) had caloric weakness.
In a series of 13 patients with Ramsay Hunt syndrome, Martin-Sanz and colleagues (Martin-Sanz, Rueda et al. 2017) reported caloric weakness of 52.5% ± 35.93%.
Testing: video head impulse testing
Martin-Sanz and colleagues (Martin-Sanz, Rueda et al. 2017) studied video head impulse testing in 18 patients with vestibular neuritis and 13 patients Ramsay Hunt syndrome. In the Ramsay Hunt syndrome patients they reported reduced vestibulo-ocular reflex gain of 0.63 ± 0.40 on the affected side. They took improvement in vestibulo-ocular reflex gain, and decrease in the latency of compensatory saccades, to reflect vestibular recovery. By these criteria, patients with Ramsay Hunt syndrome recovered vestibular function more poorly than those with vestibular neuritis.
Testing: other ocular motor testing
Kim and colleagues (Kim, Jeong et al. 2015) studied a series of 17 patients with Ramsay Hunt syndrome who complained of disequilibrium, and reported that 94% exhibited vibration-induced nystagmus and 59% exhibited hyperventilation-induced nystagmus.
Testing: cervical vestibular evoked myogenic potentials
In a series of 10 patients with Ramsay Hunt syndrome, Ozeki and colleagues (Ozeki, Iwasaki et al. 2006) reported that 7 (70%) exhibited abnormalities in air-conducted cervical vestibular evoked myogenic potentials.
Takahashi and colleagues (Takahashi, Sato et al. 2021) studied a series of patients with Ramsay Hunt syndrome and reported that 3/18 (17%) had abnormal cervical vestibular evoked myogenic potentials.
Testing: ocular vestibular evoked myogenic potentials
Takahashi and colleagues (Takahashi, Sato et al. 2021) studied a series of patients with Ramsay Hunt syndrome and reported that 9/17 (53%) had abnormal ocular vestibular evoked myogenic potentials.
Imaging
MRI of the internal auditory canals may show T2/FLAIR signal abnormalities and enhancement of the vestibulocochlear and facial nerves (Hasuike, Sekitani et al. 1995, Chung, Lee et al. 2015, Takahashi, Sato et al. 2021).
The series studied by Iwasaki and colleagues (Iwasaki, Toda et al. 2013) reported that of 12 patients with caloric weakness, 11 (92%) showed enhancement of the superior division of the ipsilateral vestibular nerve. Of all 14 patients with lower motor neuron facial weakness, only 4 (29%) showed enhancement of the ipsilateral facial nerve.
Some studies report enhancement in brainstem nuclei (Inagaki et al. 2018; Kim et al. 2007; Yacovino et al. 2023) or cerebellum (Sartoretti-Schefer, Kollias et al. 1999, Mizock, Bartt et al. 2000, Letchuman and Donohoe 2019), suggesting that some cases may involve a component of encephalitis. Sun and colleagues (Sun, You et al. 2022) reported a case of Ramsay Hunt syndrome associated with infarction secondary to “vertebral artery vasculopathy” (perhaps VZV vasculitis).
Diagnostic testing overall
The Table below summarizes the test results reported in the studies discussed above.
|
Test |
Iwasaki et al. (Iwasaki, Toda et al. 2013) |
Wayman et al. (Wayman, Pham et al. 1990) |
Takahashi et al. (Takahashi, Sato et al. 2021) |
Ozeki et al. (Ozeki, Iwasaki et al. 2006) |
Kim et al. (Kim, Choi et al. 2016) |
|
Audiometry showing hearing loss |
71% |
19% |
76% |
||
|
Caloric weakness |
86% |
— |
79% |
100% |
— |
|
Weakness on cervical VEMP |
— |
— |
17% |
70% |
— |
|
Weakness on ocular VEMP |
— |
— |
53% |
— |
— |
Table : Table comparing data of test results from multiple studies of patients with Ramsay Hunt syndrome.
Treatment
Attempted treatments have included oral steroids and anti-viral agents. Steroids have included methylprednisolone (Iwasaki, Toda et al. 2013) and prednisone (Robillard, Hilsinger et al. 1986). Anti-viral agents have included valacyclovir (Iwasaki, Toda et al. 2013) and acyclovir (Goswami and Gaurkar 2023). Evidence supporting these treatments is weak.
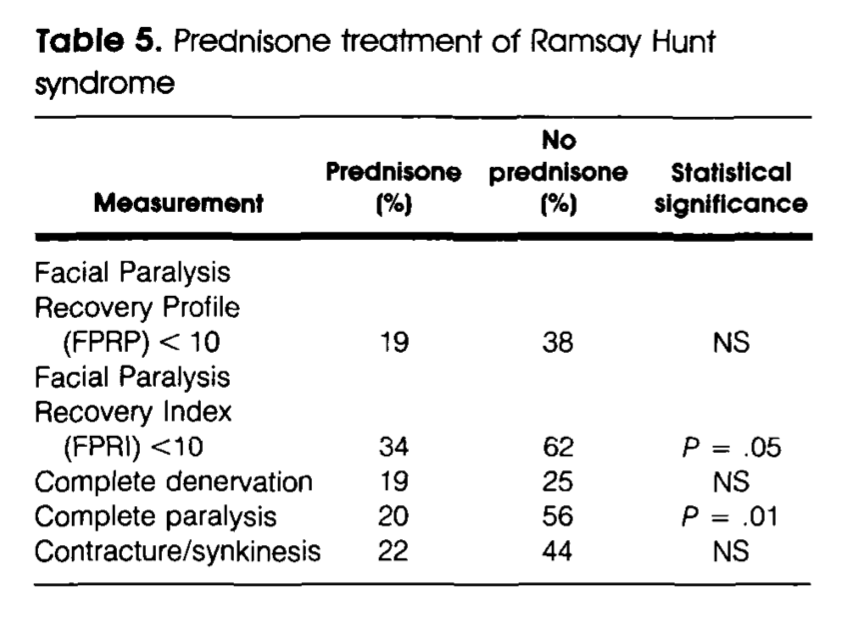
In the series of Ramsay Hunt syndrome patients studied by Robillard and colleagues (Robillard, Hilsinger et al. 1986), treatment with oral prednisone modestly improved recovery from facial paralysis, as shown in the Table below.
As far as the vestibular symptoms are concerned, since RHS causes vestibular weakness, it is logical to offer vestibular rehabilitation therapy, though there are few reports on outcomes of this treatment specifically for RHS (Gill-Body et al. 1994; Liao et al. 2011).
Prognosis
Despite treatment with oral prednisone, outcomes from facial paralysis are still poorer than in patients with Bell’s palsy (Robillard, Hilsinger et al. 1986, Lee, Chae et al. 2006).
Martin-Sanz and colleagues (Martin-Sanz, Rueda et al. 2017) the presence of facial palsy was a predictor of the severity of the initial impairment in the vestibulo-ocular reflex (VOR) of video head impulse testing, but the facial paralysis did not correlate with the final VOR (in other words, it did not predict recovery of vestibular function).
A Cochrane review (Uscategui, Doree et al. 2008) found no difference in outcomes for Ramsay Hunt syndrome patients treated with anti-viral agents (acyclovir, valacyclovir, famciclovir, brivudin).
Overall, prognosis in children is worse than in adults (Kansu and Yilmaz 2012), though recovery from facial weakness may be better (Hato, Kisaki et al. 2000).
References
Adour, K. K. (1994). “Otological complications of herpes zoster.” Ann Neurol 35 Suppl: S62-64.
Chung, M. S., J. H. Lee, D. Y. Kim, Y. M. Lim, J. H. Ahn, Y. S. Sung, Y. J. Choi, R. G. Yoon and J. H. Baek (2015). “The clinical significance of findings obtained on 3D-FLAIR MR imaging in patients with Ramsay-Hunt syndrome.” Laryngoscope 125(4): 950-955.
Coulson, S., G. R. Croxson, R. Adams and V. Oey (2011). “Prognostic factors in herpes zoster oticus (ramsay hunt syndrome).” Otol Neurotol 32(6): 1025-1030.
Gill-Body KM, Krebs DE, Parker SW, Riley PO (1994) Physical therapy management of peripheral vestibular dysfunction: two clinical case reports. Phys Ther 74: 129-42. doi: 10.1093/ptj/74.2.129
Goswami, Y. and S. S. Gaurkar (2023). “Ramsay Hunt Syndrome: An Introduction, Signs and Symptoms, and Treatment.” Cureus 15(1): e33688.
Hasuike, K., T. Sekitani and Y. Imate (1995). “Enhanced MRI in patients with vestibular neuronitis.” Acta Otolaryngol Suppl 519: 272-274.
Hato, N., H. Kisaki, N. Honda, K. Gyo, S. Murakami and N. Yanagihara (2000). “Ramsay Hunt syndrome in children.” Ann Neurol 48(2): 254-256.
Hunt, J. R. (1907). “On herpetic inflammations of the geniculate gangion. A new syndrome and its complicaitons.” The Journal of Nervous and Mental Disease 34(2).
Inagaki, A., T. Toyoda, M. Mutou and S. Murakami (2018). “Ramsay Hunt syndrome associated with solitary nucleus, spinal trigeminal nucleus and tract, and vestibular nucleus involvement on sequential magnetic resonance imaging.” J Neurovirol 24(6): 776-779.
Iwasaki, H., N. Toda, M. Takahashi, T. Azuma, K. Nakamura, S. Takao, M. Harada and N. Takeda (2013). “Vestibular and cochlear neuritis in patients with Ramsay Hunt syndrome: a Gd-enhanced MRI study.” Acta Otolaryngol 133(4): 373-377.
Kansu, L. and I. Yilmaz (2012). “Herpes zoster oticus (Ramsay Hunt syndrome) in children: case report and literature review.” Int J Pediatr Otorhinolaryngol 76(6): 772-776.
Kim, C. H., H. Choi and J. E. Shin (2016). “Characteristics of hearing loss in patients with herpes zoster oticus.” Medicine (Baltimore) 95(46): e5438.
Kim, C. H., J. W. Choi, K. J. Han, Y. S. Lee and J. E. Shin (2018). “Direction-fixed and Direction-changing Positional Nystagmus in Ramsay Hunt Syndrome.” Otol Neurotol 39(3): e209-e213.
Kim, C. H., K. H. Jeong, S. H. Ahn, D. H. Shin, Y. W. Kim and J. E. Shin (2015). “Vibration- and hyperventilation-induced nystagmus in patients with Ramsay Hunt syndrome with vertigo.” Otolaryngol Head Neck Surg 152(5): 912-918.
Kim, J. H., P. W. Chung, S. Oh, S. B. Hong, C. S. Chung, C. W. Jung, S. T. Kim, S. D. Hong and D. W. Seo (2007). “Ramsay Hunt syndrome complicated by a brainstem lesion.” J Clin Virol 39(4): 322-325.
Kuhweide, R., V. Van de Steene, S. Vlaminck and J. W. Casselman (2002). “Ramsay Hunt syndrome: pathophysiology of cochleovestibular symptoms.” J Laryngol Otol 116(10): 844-848.
Lee, D. H., S. Y. Chae, Y. S. Park and S. W. Yeo (2006). “Prognostic value of electroneurography in Bell’s palsy and Ramsay-Hunt’s syndrome.” Clin Otolaryngol 31(2): 144-148.
Lee, J., B. Choi, H. Noh, H. Jeong, J. E. Shin and C. H. Kim (2021). “Nystagmus in Ramsay Hunt syndrome with or without dizziness.” Neurol Sci 42(1): 193-198.
Letchuman, V. and C. D. Donohoe (2019). “Brainstem and Cerebellar Involvement in Ramsay Hunt Syndrome.” Case Rep Otolaryngol 2019: 7605056.
Liao WL, Sung PY, Chui WF, Chang TP (2011) Vestibular rehabilitation therapy in a patient with chronic vestibulopathy of ramsay hunt syndrome. Am J Phys Med Rehabil 90: 851-5. doi: 10.1097/PHM.0b013e3182240bec
Martin-Sanz, E., A. Rueda, J. Esteban-Sanchez, J. Yanes, J. Rey-Martinez and R. Sanz-Fernandez (2017). “Vestibular Restoration and Adaptation in Vestibular Neuritis and Ramsay Hunt Syndrome With Vertigo.” Otol Neurotol 38(7): e203-e208.
Mizock, B. A., R. Bartt and B. Agbemazdo (2000). “Herpes zoster oticus with pontine lesion: segmental brain-stem encephalitis.” Clin Infect Dis 30(1): 229-230.
Ozeki, H., S. Iwasaki, M. Ushio, N. Takeuchi and T. Murofushi (2006). “The lesion site of vestibular dysfunction in Ramsay Hunt syndrome: a study by click and galvanic VEMP.” J Vestib Res 16(4-5): 217-222.
Rhoton, A. L., Jr., S. Kobayashi and W. H. Hollinshead (1968). “Nervus intermedius.” J Neurosurg 29(6): 609-618.
Robillard, R. B., R. L. Hilsinger, Jr. and K. K. Adour (1986). “Ramsay Hunt facial paralysis: clinical analyses of 185 patients.” Otolaryngol Head Neck Surg 95(3 Pt 1): 292-297.
Sartoretti-Schefer, S., S. Kollias and A. Valavanis (1999). “Ramsay Hunt syndrome associated with brain stem enhancement.” AJNR Am J Neuroradiol 20(2): 278-280.
Sun, H., H. You and H. Wu (2022). “Brainstem Infarction and Vertebral Artery Vasculopathy After Ramsay Hunt Syndrome.” Neurology 98(21): 890-891.
Takahashi, M., G. Sato, N. Toda, T. Azuma, K. Nakamura, H. Iwasaki, H. Miyoshi, K. Matsuda, Y. Kitamura, K. Abe, S. Takao, M. Harada and N. Takeda (2021). “Vestibular and cochlear nerve enhancement on MRI and its correlation with vestibulocochlear functional deficits in patients with Ramsay Hunt syndrome.” Auris Nasus Larynx 48(3): 347-352.
Uscategui, T., C. Doree, I. J. Chamberlain and M. J. Burton (2008). “Antiviral therapy for Ramsay Hunt syndrome (herpes zoster oticus with facial palsy) in adults.” Cochrane Database Syst Rev 2008(4): CD006851.
Wayman, D. M., H. N. Pham, F. M. Byl and K. K. Adour (1990). “Audiological manifestations of Ramsay Hunt syndrome.” J Laryngol Otol 104(2): 104-108.
Yacovino DA, Perez Akly MS, Ibanez T, Cherchi M (2023) Vestibular Nucleus Involvement in Patients With Acute Vertigo Due to Herpes Zoster Oticus or Vestibular Neuritis. Neurology. doi: 10.1212/WNL.0000000000207549
![]()