By Marcello Cherchi, MD PhD
For patients
See-saw nystagmus (SSN) is a disorder in which the eyes move in a “see-saw” like pattern. Most cases begin in adulthood, though some appear in infancy. The underlying cause of SSN is unknown, though many patients are found to have limited vision. A patient with SSN usually gets a brain MRI and consults with an ophthalmologist or neuro-ophthalmologist.
For clinicians
Overview
See-saw nystagmus (SSN) is a rare eye movement disorder in which the eyes move in a see-saw pattern, meaning that there is a cycle of pendular nystagmus in which (1) one eye lowers and extorts while the other eye simultaneously rises and intorts, then (2) the first eye rises and intorts while the other eye simultaneously lowers and extorts. The term “hemi-see-saw” nystagmus refers to a pattern that is similar except that part of the cycle is slow (pendular nystagmus) and part of the cycle is fast (jerk nystagmus). SSN can be congenital or acquired. The mechanism is unknown. Usually, it occurs in the context of visual deficits; less commonly it occurs in individuals whose vision is intact. Many (though not all) patients are found to have a disorder at the optic chiasm (typically associated with bitemporal hemianopsia). A smaller proportion of patients have pathology involving the brainstem (such as infarction). In a patient with SSN it is appropriate to check imaging (brain MRI) and refer for an ophthalmologic and/or neuro-ophthalmologic evaluation. Treatment and prognosis depend on the underlying etiology; for example, in a patient with a tumor compressing the optic chiasm, resection of the tumor may bring about some improvement. There are a few reported cases of SSN improving with clonazepam.
Introduction
The British ophthalmologist, Dr. Ernest Edmund Maddox (1863 – 1933) (Cooper 1934) was the first to describe see-saw nystagmus (Maddox 1914). Since then, dozens of cases have been reported in the literature.
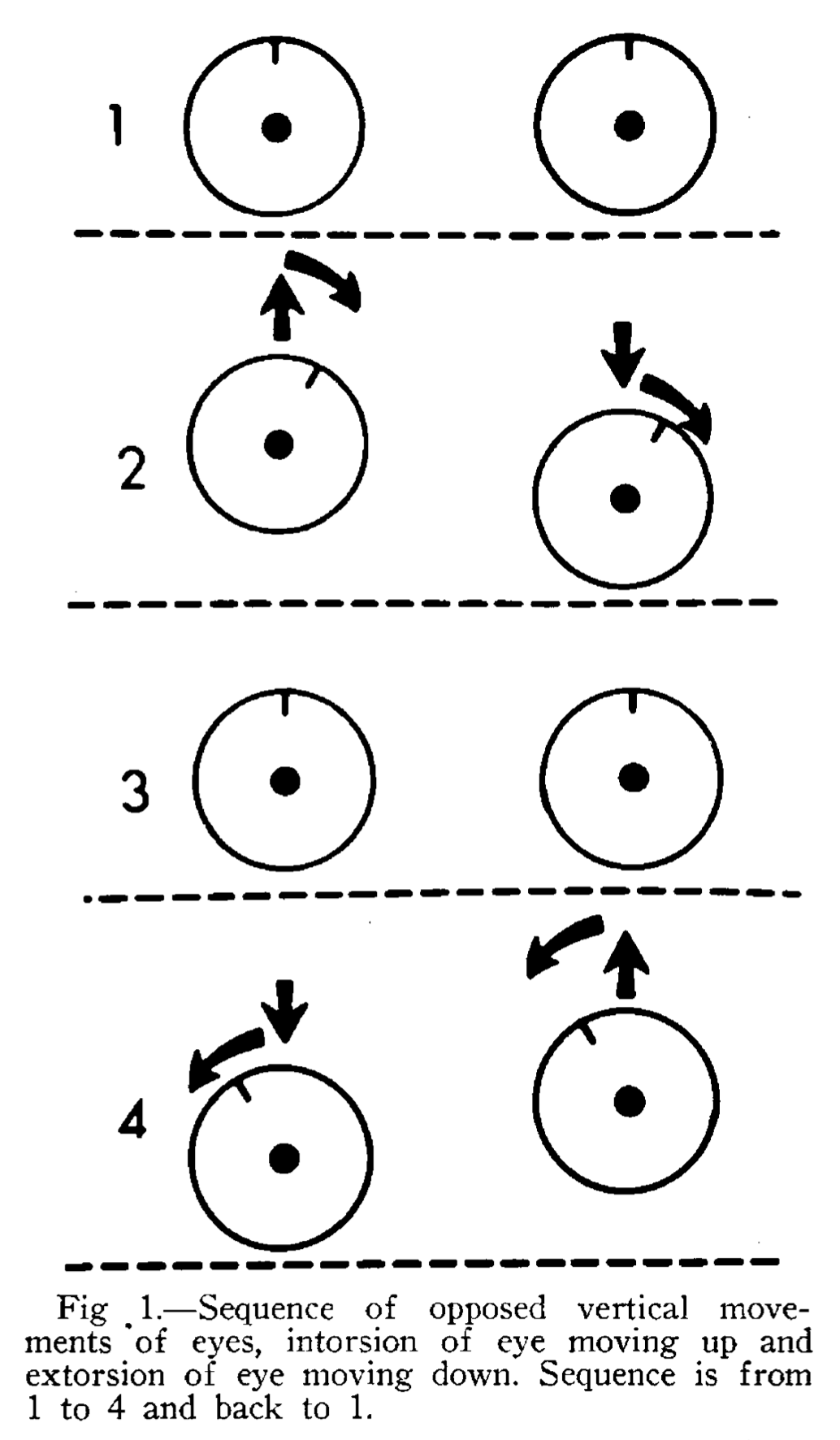
The term see-saw nystagmus (SSN) refers to a dysconjugate eye movement abnormality in which (1) the first eye rises and intorts while the fellow eye lowers and extorts; (2) the first eye lowers and extorts, while the fellow eye rises and intorts; (3) the cycle repeats. This movement is said to resemble that of a see-saw with its fulcrum at the nasal bridge.
The Figure below, from Druckman and colleagues (Druckman et al. 1966), illustrates the cycle of see-saw nystagmus.
The nomenclature for see-saw nystagmus is confusing. The unqualified term “see-saw nystagmus” refers to a situation in which the described eye movements are slow (pendular) throughout their entire cycle. In contrast, the term “hemi-see-saw nystagmus” refers to the same eye movement when the initial eccentric movement (vertical and torsional) is slow (similar to the pendular variety), but the return to primary position of gaze is fast (jerk nystagmus); in other words, only half of the cycle (“hemi”) is pendular nystagmus, while the other half is jerk nystagmus. Contrary to what one might expect, note that the term “hemi-see-saw nystagmus” does not refer to a situation in which only one eye exhibits this pattern.
Epidemiology
See-saw nystagmus (SSN) is rare, though its incidence and prevalence are unknown.
Several articles include summary reviews of previously published cases (Drachman 1966; Druckman et al. 1966; Fein and Williams 1969; Nakada and Kwee 1988).
Most cases of see-saw nystagmus (SSN) are acquired. Occasional congenital cases have been reported, usually in patients with congenital optic chiasm abnormalities (Apkarian and Bour 2001; Nguyen et al. 2018) or congenital retinitis pigmentosa (Bergin and Halpern 1986).
Some cases of SSN occur in the context of blindness (Jeong et al. 2009) or significant visual loss from retinitis pigmentosa (RP), whether the onset of visual loss is in childhood (Bergin and Halpern 1986) or adulthood (Chiew 2023).
Some cases of SSN occur in the context of congenital optic chiasm defects, usually achiasma (Nguyen et al. 2018), hemichiasma (Dell’Osso and Daroff 1998) or chiasmic dysplasia (Davis and Shock 1975) such as optic fiber non-decussation (Apkarian and Bour 2001; Davis and Shock 1975). In other cases the optic chiasm has been damaged, typically by compression from a space-occupying lesion (Daroff 1965) such as craniopharyngioma (Druckman et al. 1966; Kinder and Howard 1963; Pal et al. 2020; Saluja et al. 2020; Schurr 1963), pituitary adenoma (Schurr 1963) or suprasellar epidermoid cyst (Smith and Mark 1959). Generally these patients with optic chiasm defects have bitemporal hemianopsia.
Some cases of acquired SSN result from infarction (Daroff 1965). Halmagyi and colleagues (Halmagyi et al. 1994) described two patients with see-saw nystagmus who had suffered left thalamic hemorrhages. Kanter and colleagues (Kanter et al. 1987) reported a case of see-saw nystagmus in a patient who had suffered a “presumed brainstem vascular event” in the paramedian ventral midbrain with “involvement of the right interstitial nucleus of Cajal.” Lee and Kim (Lee and Kim 2018) describe see-saw nystagmus in a patient who had suffered an infarction involving the left anterior rostral cerebellar hemisphere and rostral vermis and superior cerebellar peduncle. Man and Fu (Man and Fu 2014) report on a patient with a paramedian thalamomesencephalic infarct who developed a combination of see-saw nystagmus, convergence-retraction nystagmus and contraversive ocular tilt.
Rarely, acquired SSN occurs in the context of multiple sclerosis (Samkoff and Smith 1994; Sandramouli et al. 2005).
One case of see-saw nystagmus has been reported in the context of a paraneoplastic syndrome (Rizvi et al. 2018) in a patient with breast cancer and antineuronal antibody type 2.
Hemi-see-saw nystagmus is less common than “plain” see-saw nystagmus, though its incidence and prevalence are unknown.
Pathophysiological mechanism of disease
The mechanism of see-saw nystagmus is unknown. Mathematical models have been proposed within control systems analysis suggesting mechanisms in specific etiologies (Nakada and Kwee 1992; Rizvi et al. 2018) or as a more general framework (Cherchi 2026), but there is still no consensus on this question.
Because many patients with SSN have significant visual defects, several investigators have proposed that the reduced visual input is key to explaining this phenomenon (Arnott 1964). For example:
“Based on analysis of the ocular oscillation characteristics of the cases of seesaw nystagmus reported in the literature… we postulate that seesaw nystagmus is another type of ocular oscillation brought about by an unstable visuovestibular interaction control system. Nonavailability of retinal error signals to the inferior olivary nucleus essential for vestibuloocular reflex adaptation due to complete chiasmal dissection makes the system less stable. This system instability is further accentuated by the pursuit feedback element. The intact inferior olivary nucleus-nodulus connections in seesaw nystagmus would explain the 180 degree phase difference that distinguishes it from the midline form of oculopalatal myoclonus, where these connections are likely disrupted” (Nakada and Kwee 1988).
And:
“Therefore, in the presence of normal labyrinthine signals, insufficient visual input via accessory optic system can adaptively increase the excitability of the INC neurons. Such maladaptive increase in excitability leads to oscillations comprising pendular seesaw nystagmus” (Rizvi et al. 2018).
Whether this proposal is correct, or at least whether it is the only mechanism of see-saw nystagmus, is brought into question by the fact that some patients with SSN have no detectable visual impairment. Rizvi and colleagues (Rizvi et al. 2018) studied a case of acquired see-saw nystagmus in the context of a paraneoplastic syndrome in a patient with breast cancer and antineuronal antibody type 2 who had no visual deficits and no cerebellar findings on examination. Using a control systems analysis, they proposed:
“The hypothesis that abnormal increases in the excitability of the INC [interstitial nucleus of Cajal] excitatory burst neurons (due to cross immune etiology) that comprise reciprocally excitatory circuit can cause reverberations leading to pendular or pendular seesaw nystagmus” (Rizvi et al. 2018).
Some cases of see-saw nystagmus have been reported following head trauma (Eggenberger 2015; Frisen and Wikkelso 1986; Nakada and Kwee 1988), and may be delayed (Eggenberger 2002; Yunusov et al. 2014). Usually such cases also involve bitemporal hemianopsia (Eggenberger 2002; Frisen and Wikkelso 1986), which may be complete or partial (Nakada and Kwee 1988), or optic atrophy (Yunusov et al. 2014). In these cases it is unclear whether the SSN results from the visual deficit, or from some other damage consequent to the head trauma.
Hemi-see-saw nystagmus has been reported following a variety of lesions, often in association with some other ocular motor abnormality.
- Choi and colleagues (Choi et al. 2009) reported a case of pontine infarction presenting with hemi-see-saw nystagmus and internuclear ophthalmoplegia.
- Choi and colleagues (Choi et al. 2004) reported a case of medial medullary infarction presenting with bowtie and upbeat nystagmus that evolved into hemi-see-saw nystagmus.
- Lee and colleagues (Lee et al. 2014) reported a case of medial medullary infarction presenting with torsion-upbeat nystagmus that later evolved into hemi-see-saw nystagmus.
- Lee and colleagues (Lee et al. 2014) reported on a patient with a medial medullary infarction who exhibited up beat torsional nystagmus that evolved into hemi-see-saw nystagmus.
- Khan and Lueck (Khan and Lueck 2013) reported hemi-see-saw nystagmus in a case of lateral medullary syndrome.
- Kim and colleagues (Kim et al. 2023) reported fixation-elicited hemi-see-saw nystagmus in a case of mesodiencephalic infarction.
- Lee and Kim (Lee and Kim 2018) reported hemi-see-saw nystagmus in a case of infarction in the territory of the superior cerebellar artery.
- Hemi-see-saw nystagmus has been reported in Joubert syndrome (Jang et al. 2020).
- Animal experimental inactivation of the interstitial nucleus of Cajal has been reported to result in hemi-see-saw nystagmus (Das et al. 2010).
Clinical presentation
The most common complaint in patients with see-saw nystagmus is visual disturbance, such as oscillopsia, and this is the usual reason for referral to otoneurology. In cases that develop in the context of slowly progressive visual loss, the patient usually is initially seen by ophthalmology.
Physical examination
Patients with isolated see-saw nystagmus usually have otherwise normal general physical and neurological examinations. However, given the frequent association with visual loss, an examiner should do a beside check of visual fields.
See-saw nystagmus can also present as part of a broader problem (see the section on differential diagnosis below), and such patients often have other abnormalities on physical examination.
Ocular motor examination
In some cases see-saw nystagmus (SSN) is subtle and may only be detectable on instrumented oculography. However, in most cases, the SSN can be observed on face-to-face examination. It may be modulated by various voluntary eye movements; for instance, it may diminish on convergence (Yunusov et al. 2014), or increase on eccentric gaze.
In many cases the eye movement is slow and thus would be classified as pendular nystagmus (Daroff 1965; Drachman 1966; Druckman et al. 1966; Porta-Etessam et al. 2009; Sandramouli et al. 2005), while in other cases it has more the quality of a jerk nystagmus (Halmagyi et al. 1994; Oh et al. 2005). See the discussion above regarding the distinction between “see-saw nystagmus” and “hemi-see-saw nystagmus.”
The Video below, from https://www.youtube.com/watch?v=ir0_mbcE-Pk (accessed 4/5/23), shows see-saw nystagmus. The vertical component of the eye movements is more obvious in this grayscale video.
The Video below, from https://www.youtube.com/watch?v=4qoKvSOc5To (accessed 4/5/23), shows see-saw nystagmus. The torsional component is more obvious in this video due to the easily visible scleral vasculature.
The Video below, from https://www.youtube.com/watch?v=EK_qPi3o4Xk (accessed 4/5/23), shows see-saw nystagmus. The vertical and torsional components are obvious. The tempo of the eye movement is slower, and thus classified as pendular rather than jerk nystagmus.
The Video below, from Rudich and Lesser (Rudich and Lesser 2009), shows see-saw nystagmus evident on face-to-face examination.
Some cases of SSN may be more difficult to recognize when the SSN occurs in conjunction with another ocular motor abnormality, such as congenital nystagmus (Apkarian and Bour 2001), bowtie nystagmus (Choi et al. 2004), internuclear ophthalmoplegia (Choi et al. 2009), latent nystagmus (“infantile nystagmus”) (Dell’Osso et al. 2007), periodic alternating nystagmus (Jeong et al. 2009) or convergence-retraction nystagmus (Man and Fu 2014). In some of these cases the SSN may develop after some other form of nystagmus (Choi et al. 2004; Lee et al. 2014).
Testing: instrumented oculography
The Figure below, from Nguyen and colleagues (Nguyen et al. 2018), shows oculographic tracings from a patient with see-saw nystagmus. The salient characteristic is that the tracings of horizontal eye movements (blue = right eye, orange = left eye) are conjugate, while the tracings of vertical eye movements (yellow = right eye, purple = left eye) are 180 degrees out of phase. Unfortunately there are no tracings for the torsional eye movements (which one would expect to be conjugate).

Differential diagnosis
See-saw nystagmus can occur in association with a number of ophthalmologic and neurologic conditions. The following list combines differential diagnoses listed in Eggenberger (Eggenberger 2002) and Leigh and Rucker (Leigh and Rucker 2005).
- Achiasma
- Albinism
- Brainstem stroke, particularly upper brainstem infarction
- Chiari malformation
- Congenital, including agenesis of the optic chiasm
- Head trauma
- Hemichiasma
- Meso-diencephalic disease
- Midbrain tumor
- Multiple sclerosis
- Parasellar masses, sometimes with extension
- Septo-optic dysplasia
- Syringobulbia
- Vision loss from retinitis pigmentosa or rod cone dystrophy
When visual symptoms develop abruptly and see-saw nystagmus is present on examination, vascular causes should be suspected and imaging (brain MRI) is appropriate.
When see-saw nystagmus is observed in a patient with a history of gradually progressive visual loss, especially if physical examination demonstrates bitemporal hemianopsia, it is appropriate to check imaging (brain MRI) in order to assess for a structural lesion compressing the optic chiasm.
Hemi-see-saw nystagmus has been reported following a variety of lesions, often in association with some other ocular motor abnormality.
- Choi and colleagues (Choi et al. 2009) reported a case of pontine infarction presenting with hemi-see-saw nystagmus and internuclear ophthalmoplegia.
- Choi and colleagues (Choi et al. 2004) reported a case of medial medullary infarction presenting with bowtie and upbeat nystagmus that evolved into hemi-see-saw nystagmus.
- Lee and colleagues (Lee et al. 2014) reported a case of medial medullary infarction presenting with torsion-upbeat nystagmus that later evolved into hemi-see-saw nystagmus.
- Lee and colleagues (Lee et al. 2014) reported on a patient with a medial medullary infarction who exhibited up beat torsional nystagmus that evolved into hemi-see-saw nystagmus.
- Khan and Lueck (Khan and Lueck 2013) reported hemi-see-saw nystagmus in a case of lateral medullary syndrome.
- Kim and colleagues (Kim et al. 2023) reported fixation-elicited hemi-see-saw nystagmus in a case of mesodiencephalic infarction.
- Lee and Kim (Lee and Kim 2018) reported hemi-see-saw nystagmus in a case of infarction in the territory of the superior cerebellar artery.
- Hemi-see-saw nystagmus has been reported in Joubert syndrome (Jang et al. 2020).
- Animal experimental inactivation of the interstitial nucleus of Cajal has been reported to result in hemi-see-saw nystagmus (Das et al. 2010).
Consultation with ophthalmology and/or neuro-ophthalmology is appropriate for all cases of see-saw nystagmus and hemi-see-saw nystagmus.
Treatment
Treatment of reversible causes of see-saw nystagmus (such as resection of a tumor compressing the optic chiasm) is appropriate. Surgical removal of a causative tumor sometimes also brings about improvement in see-saw nystagmus (Kinder and Howard 1963; Mark et al. 1960; Pal et al. 2020; Smith and Mark 1959). In some cases the post-surgical improvement is transient, and the see-saw nystagmus eventually returns (Schurr 1963).
There are several case reports of see-saw nystagmus improving with clonazepam (Cochin et al. 1995; Eggenberger 2002), sometimes in combination with baclofen (Eggenberger 2002).
Some reports notice transient diminution of see-saw nystagmus after ingestion of alcohol (Frisen and Wikkelso 1986).
Prognosis
Prognosis of see-saw nystagmus depends on its etiology.
References
Apkarian P, Bour LJ (2001) See-saw nystagmus and congenital nystagmus identified in the non-decussating retinal-fugal fiber syndrome. Strabismus 9: 143-63. doi: 10.1076/stra.9.3.143.6761
Arnott EJ (1964) Vertical see-saw nystagmus. Trans Ophthalmol Soc U K (1962) 84: 251-7.
Bergin DJ, Halpern J (1986) Congenital see-saw nystagmus associated with retinitis pigmentosa. Ann Ophthalmol 18: 346-9.
Cherchi M (2026) A model of see-saw nystagmus. Journal of Neurology 273: 427. doi: 10.1007/s00415-026-13956-1
Chiew YR (2023) See Saw Nystagmus Associated with Retinitis Pigmentosa. QJM. doi: 10.1093/qjmed/hcad052
Choi KD, Jung DS, Park KP, Jo JW, Kim JS (2004) Bowtie and upbeat nystagmus evolving into hemi-seesaw nystagmus in medial medullary infarction: possible anatomic mechanisms. Neurology 62: 663-5. doi: 10.1212/01.wnl.0000110186.05217.9b
Choi SY, Kim DH, Lee JH, Kim J (2009) Jerky hemi-seesaw nystagmus and head tilt reaction combined with internuclear ophthalmoplegia from a pontine infarction. J Clin Neurosci 16: 456-8. doi: 10.1016/j.jocn.2008.03.015
Cochin JP, Hannequin D, Do Marcolino C, Didier T, Augustin P (1995) [Intermittent sea-saw nystagmus successfully treated with clonazepam]. Rev Neurol (Paris) 151: 60-2.
Cooper JB (1934) Dr. Ernest E. Maddox. British Journal of Ophthalmology 18: 55. doi: 10.1136/bjo.18.1.55
Daroff RB (1965) See-Saw Nystagmus. Neurology 15: 874-7. doi: 10.1212/wnl.15.9.874
Das VE, Leigh RJ, Swann M, Thurtell MJ (2010) Muscimol inactivation caudal to the interstitial nucleus of Cajal induces hemi-seesaw nystagmus. Exp Brain Res 205: 405-13. doi: 10.1007/s00221-010-2376-2
Davis GV, Shock JP (1975) Septo-optic dysplasia associated with see-saw nystagmus. Arch Ophthalmol 93: 137-9. doi: 10.1001/archopht.1975.01010020143011
Dell’Osso LF, Daroff RB (1998) Two additional scenarios for see-saw nystagmus: achiasma and hemichiasma. J Neuroophthalmol 18: 112-3.
Dell’Osso LF, Jacobs JB, Serra A (2007) The sub-clinical see-saw nystagmus embedded in infantile nystagmus. Vision Res 47: 393-401. doi: 10.1016/j.visres.2006.09.001
Drachman DA (1966) See-saw nystagmus. J Neurol Neurosurg Psychiatry 29: 356-61. doi: 10.1136/jnnp.29.4.356
Druckman R, Ellis P, Kleinfeld J, Waldman M (1966) Seesaw nystagmus. Arch Ophthalmol 76: 668-75. doi: 10.1001/archopht.1966.03850010670008
Eggenberger ER (2002) Delayed-onset seesaw nystagmus posttraumatic brain injury with bitemporal hemianopia. Ann N Y Acad Sci 956: 588-91. doi: 10.1111/j.1749-6632.2002.tb02890.x
Eggenberger ER (2015) Mystery Case: Pendular see-saw nystagmus as a delayed complication of traumatic brain injury. Neurology 84: 547. doi: 10.1212/01.wnl.0000461046.30280.e4
Fein JM, Williams DB (1969) See-saw nystagmus. J Neurol Neurosurg Psychiatry 32: 202-7. doi: 10.1136/jnnp.32.3.202
Frisen L, Wikkelso C (1986) Posttraumatic seesaw nystagmus abolished by ethanol ingestion. Neurology 36: 841-4. doi: 10.1212/wnl.36.6.841
Halmagyi GM, Aw ST, Dehaene I, Curthoys IS, Todd MJ (1994) Jerk-waveform see-saw nystagmus due to unilateral meso-diencephalic lesion. Brain 117 ( Pt 4): 789-803. doi: 10.1093/brain/117.4.789
Jang SH, Choi SY, Jeon H, Choi HY, Oh EH, Choi JH, Choi KD (2020) Hemi-seesaw Nystagmus in Joubert Syndrome. Can J Neurol Sci 47: 270-272. doi: 10.1017/cjn.2019.343
Jeong SH, Hwang JM, Kim JS (2009) Co-occurrence of periodic alternating and pendular seesaw nystagmus in blindness. J Neurol Sci 285: 257-8. doi: 10.1016/j.jns.2009.06.042
Kanter DS, Ruff RL, Leigh RJ, Modic M (1987) See-saw nystagmus and brainstem infarction: MRI findings. Neuroophthalmology 7: 279-83. doi: 10.3109/01658108708996003
Khan SR, Lueck CJ (2013) Hemi-seesaw nystagmus in lateral medullary syndrome. Neurology 80: 1261-2. doi: 10.1212/WNL.0b013e318289dcbe
Kim HS, Oh EH, Choi J-H (2023) Visual Fixation-Induced Hemi-Seesaw Nystagmus. Res Vestib Sci 22: 19-22. doi: 10.21790/rvs.2023.22.1.19
Kinder RS, Howard GM (1963) See-Saw Nystagmus. An Unusual Sign of Lesions near the Third Ventricle. Am J Dis Child 106: 331-2.
Lee H, Kim HA (2018) Hemi-seesaw nystagmus in a patient with acute infarction in the superior cerebellar artery territory. J Neurol 265: 1219-1221. doi: 10.1007/s00415-018-8839-2
Lee SU, Park SH, Jeong SH, Kim HJ, Kim JS (2014) Evolution of torsional-upbeat into hemi-seesaw nystagmus in medial medullary infarction. Clin Neurol Neurosurg 118: 80-2. doi: 10.1016/j.clineuro.2014.01.003
Leigh JR, Rucker JC (2005) Nystagmus and related ocular motility disorders. In: Miller NR, Newman NJ (eds) Walsh & Hoyt’s Clinical Neuro-Ophthalmology, 6th edition edn, vol 1. Lippincott Williams & Wilkins, 530 Walnut Street, Philadelphia, Pennsylvania 19106 USA; 351 West Camden Street, Baltimore, Maryland 21201-2436 USA, pp 1133-1173
Maddox EE (1914) See-saw nystagmus with bitemporal hemianopia. Proc R Soc Med 7: 12-13.
Man BL, Fu YP (2014) See-saw nystagmus, convergence-retraction nystagmus and contraversive ocular tilt reaction from a paramedian thalamomesencephalic infarct. BMJ Case Rep 2014. doi: 10.1136/bcr-2014-206851
Mark VH, Smith JL, Kjellberg RD (1960) Suprasellar epidermoid tumor. A case report with the presenting complaint of see-saw nystagmus. Neurology 10: 81-3. doi: 10.1212/wnl.10.1.81
Nakada T, Kwee IL (1988) Seesaw nystagmus. Role of visuovestibular interaction in its pathogenesis. J Clin Neuroophthalmol 8: 171-7.
Nguyen CT, Goh C, Desmond P, Abel LA, Lim CHL, Andrew Symons RC, Hardy TG (2018) Congenital achiasma and see-saw nystagmus in VATER syndrome association with hydrocephalus. J Clin Neurosci 51: 63-65. doi: 10.1016/j.jocn.2018.02.008
Oh K, Chang JH, Park KW, Lee DH, Choi KD, Kim JS (2005) Jerky seesaw nystagmus in isolated internuclear ophthalmoplegia from focal pontine lesion. Neurology 64: 1313-4. doi: 10.1212/01.WNL.0000156905.31773.E1
Pal R, Dutta P, Chatterjee D, Ahuja C, Singh A (2020) Pendular See-Saw Nystagmus: A Rare Presenting Manifestation of Craniopharyngioma. Neuroophthalmology 45: 126-129. doi: 10.1080/01658107.2019.1693602
Porta-Etessam J, Casanova I, Pajuelo B, Di Capua D, del Val J, Garcia ME, Marcos A (2009) See-saw nystagmus in a patient with Wallenberg syndrome. J Neuroophthalmol 29: 73-4. doi: 10.1097/WNO.0b013e3181989dc1
Rizvi MT, Cameron L, Kilbane C, Shaikh AG (2018) Paraneoplastic seesaw nystagmus and opsoclonus provides evidence for hyperexcitable reciprocally innervating mesencephalic network. J Neurol Sci 390: 239-245. doi: 10.1016/j.jns.2018.05.002
Rudich DS, Lesser RL (2009) See-saw nystagmus in a patient with septo-optic dysplasia. J Neuroophthalmol 29: 251-2. doi: 10.1097/WNO.0b013e3181b21099
Saluja G, Samdani A, Bhatia P (2020) See-saw nystagmus in giant craniopharyngioma. BMJ Case Rep 13. doi: 10.1136/bcr-2020-235435
Samkoff LM, Smith CR (1994) See-saw nystagmus in a patient with clinically definite MS. Eur Neurol 34: 228-9. doi: 10.1159/000117044
Sandramouli S, Benamer HT, Mantle M, Chavan R (2005) See-saw nystagmus as the presenting sign in multiple sclerosis. J Neuroophthalmol 25: 56-7. doi: 10.1097/00041327-200503000-00018
Schurr PH (1963) See-Saw Nystagmus. Proc R Soc Med 56: 808-10.
Smith JL, Mark VH (1959) See-saw nystagmus with suprasellar epidermoid tumor. AMA Arch Ophthalmol 62: 280-3. doi: 10.1001/archopht.1959.04220020106015
Yunusov F, Park JH, Huh YE, Kim HJ, Kim JS (2014) Mystery Case: pendular see-saw nystagmus as a delayed complication of traumatic brain injury. Neurology 82: e147-8. doi: 10.1212/WNL.0000000000000358
![]()