By Marcello Cherchi, MD PhD
For patients
Sjögren syndrome (SS) is an autoimmune disease that can cause dry eyes, dry mouth and arthritis. Less common symptoms include hearing loss and disequilibrium. If your doctor suspects SS, then they may order several tests. Diagnosis and management is usually overseen by a rheumatologist.
For clinicians
Overview
Sjögren syndrome (SS) is an autoimmune mediated exocrinopathy and vasculopathy that was classically described as causing dry eyes (from keratoconjunctivitis sicca), dry mouth (from salivary gland dysfunction) and arthritis, though it can involve many other organ systems. It is the second most common systemic autoimmune disease (after rheumatoid arthritis), with geographic variability ranging from 0.1% – 4.8% of the population. It is significantly more common in women, with a female:male ratio ranging from 9:1 to 14:1. Numerous genetic loci have been implicated. Patients with SS may experience auditory symptoms (hearing loss) and/or vestibular symptoms (disequilibrium). On audiometry the hearing loss is generally high frequency and sensorineural. In SS patients experiencing disequilibrium, potential contributors (attributable to SS) include peripheral somatosensory neuropathy, autonomic neuropathy and vestibular weakness. Vestibular workup may show caloric weakness, prolonged cVEMP n1 latency, enlarged oVEMP p1n1 amplitude, and low gain on vHIT of the lateral and posterior semicircular canals. SS patients with hearing loss can be referred to audiology for amplification. SS patients with disequilibrium found to have evidence of vestibular weakness can be referred to vestibular rehabilitation therapy (VRT). Management of a patient with Sjögren syndrome is overseen by a rheumatologist, and requires a multidisciplinary approach when multiple organ systems are involved. Prognosis is variable.
Introduction
Henrik Samuel Conrad Sjögren (1899 – 1986) was a Swedish ophthalmologist.
In 1930 Dr. Sjögren began reporting on patients exhibiting a syndromic triad of dry eyes, dry mouth and arthritis (Sjögren 1930, 1933). These observations built on those of previous researchers (Baldini and Bombardieri 2016; Ghafoor 2012; Jonsson 2021) who reported “pairs” of these findings, such as:
- In 1888 the British physician, Hadden (1856 – 1893), reported on patients exhibiting dry eyes (xerophthalmia) and dry mouth (xerostomia) (Hadden 1888).
- In 1888 the Polish surgeon, Johann Freiharr Mikulicz-Radecki (1850 – 1905), reported on patients exhibiting enlargement of lacrimal and salivary glands (Mikulicz-Radecki 1888, 1892).
- In 1890 the French dermatologist, Henri Gourgerot (1881 – 1955), reported on systemic findings in patients with dry eyes (Gougerot 1890).
- In 1927 Mulock-Houwer reported on an association between filamentary keratitis and arthritis (Mulock-Houwer 1927).
Sjögren syndrome (SS) is now defined as the combination of keratoconjunctiva sicca, xerostomia and polyarthritis.
Epidemiology
Sjögren syndrome (SS) is the second most common systemic autoimmune disorder (after rheumatoid arthritis). The reported prevalence is geographically variable by over an order of magnitude, ranging from 0.1% to 4.8% (Mavragani and Moutsopoulos 2010). It is significantly more common in women, with a female:male ratio ranging from 9:1 (Mavragani and Moutsopoulos 2010) to 14:1 (Thorlacius et al. 2023).
Genetics
The number of genetic loci associated with primary Sjögren syndrome is large and growing, as shown in the Table below from Thorlacius and colleagues (Thorlacius et al. 2023).
|
Variant |
Position (Chr:bp) |
Gene |
Function |
Odds ratio |
P value |
|
rs7523907 |
1:167427247 |
CD247 |
T cell receptor signaling |
0.85 |
9.33 × 10−9 a |
|
rs10168266 |
2:191071078 |
STAT4 |
Intracellular signaling |
1.44 |
2 × 10−17 |
|
rs2293765 |
2:191520845 |
NAB1 |
Transcriptional repression |
1.24 |
5.53 × 10−14 |
|
rs485497 |
3:160001345 |
IL12A |
The 35-kDa subunit of IL-12 |
1.3 |
1 × 10−10 |
|
rs6579837 |
5:151055333 |
TNIP1 |
Inhibits NF-κB activation |
1.43 |
3 × 10−8 |
|
rs2431697 |
5:159879978 |
PTTG1 |
Anaphase-promoting complex substrate |
0.83 |
3.33 × 10−9 |
|
MIR146A |
Post-transcriptional regulation of gene expression |
||||
|
rs6457374 |
6:31272261 |
HLA-B |
Presents peptides derived from the endoplasmic reticulum lumen |
3.27 |
3.52 × 10−27 |
|
rs2523607 |
6:31322790 |
HLA-B |
Presents peptides derived from the endoplasmic reticulum lumen |
5.27 |
5.30 × 10−58 |
|
MICA*008 |
6:31371356 |
MICA |
Stress-induced ligand for the natural killer cell-activating protein NKG2D |
2.24 |
2.61 × 10−35 |
|
rs1800629 |
6:31543031 |
TNF |
Multifunctional pro-inflammatory cytokine |
2 |
2.48 × 10−10 |
|
rs7197 |
6:32412580 |
HLA-DRA |
Presents peptides derived from extracellular proteins |
1.56 |
2.6 × 10−25 |
|
rs116232857 |
6:32597064 |
Intergenic (HLA-DQA1 and HLA-DRB1) |
Presents peptides derived from extracellular proteins |
2.42 |
1.14 × 10−67 |
|
Presents peptides derived from extracellular proteins |
|||||
|
rs115575857 |
6:32659645 |
HLA-DQA1 |
Presents peptides derived from extracellular proteins |
3.65 |
3.7 × 10−90 |
|
HLA-DQB1 |
|||||
|
HLA-DRA |
|||||
|
rs9277464 |
6:33053352 |
HLA-DPB1 |
Presents peptides derived from extracellular proteins |
1.65 |
3 × 10−7 |
|
rs4282438 |
6:33072172 |
Intergenic (HLA-DPB2) |
Presents peptides derived from extracellular proteins |
1.58 |
8.77 × 10−25 |
|
rs5029939 |
6:137874586 |
TNFAIP3 |
Inhibits NF-κB activation |
1.67 |
8 × 10−9 |
|
rs526531 |
6:138243700 |
PRDM1 |
Repressor of IFNβ expression |
1.13 |
4.86 × 10−8 a |
|
ATG5 |
Involved in autophagic vesicle formation |
||||
|
rs4917129 |
7:50323074 |
IKZF1 |
Transcription factor that regulates lymphocyte differentiation |
0.7 |
4.24 × 10−8 |
|
rs117026326 |
7:74711703 |
GTF2I |
Phosphoprotein with roles in transcription and signal transduction |
2.2 |
1 × 10−53 |
|
NCF1 |
Subunit of neutrophil enzyme NADPH oxidase |
||||
|
rs3757387 |
7:128936032 |
IRF5 |
Transcription factor with diverse roles |
1.44 |
3 × 10−19 |
|
rs17339836 |
7:129041008 |
TNPO3 |
Nuclear import receptor |
1.58 |
2 × 10−16 |
|
rs4841466 |
8:10829159 |
XKR6 |
Unknown |
1.17 |
3.77 × 10−8 |
|
rs2736345 |
8:11494976 |
BLK |
Tyrosine kinase involved in B cell development |
1.3 |
5 × 10−10 |
|
FAM167A |
Unknown |
||||
|
rs7119038 |
11:118867572 |
CXCR5 |
Receptor for the chemokine CXCL13 |
1.35 |
1 × 10−8 |
|
rs10774671 |
12:113356943 |
OAS1 |
Interferon-induced antiviral enzyme |
0.75 |
2.59 × 10−9 |
|
rs8071514 |
17:10462513 |
RPTOR |
Controls mTORC1 activity involved in cell growth and survival |
0.84 |
1.64 × 10−8 |
|
CHMP6 |
Probably involved in the biosynthesis of endosomes |
||||
|
BAIAP2 |
Adapter protein that links membrane-bound small G proteins to cytoplasmic effector proteins. |
||||
|
rs7210219 |
17:78964083 |
MAPT |
Promotes microtubule assembly and stability |
0.78 |
2.4 × 10−10 |
|
CRHR1 |
A receptor that binds to corticotropin-releasing hormones |
||||
|
rs11085725 |
19:39747780 |
TYK2 |
Involved in interferon and cytokine signaling |
0.78 |
7.17 × 10−13 |
|
rs2069235 |
22:39747530 |
SYNGR1 |
Unknown |
1.21 |
5.06 × 10−10 |
Table : Genetic loci associated with primary Sjögren syndrome through genome-wide association studies. From Thorlacius et al. (Thorlacius et al. 2023).
Pathophysiological mechanism of disease
The etiology of SS is unknown, but “immune-mediated vasculopathy, vasculitis or demyelination are considered to be important underlying factors in the pathogenesis” (Ulusoy et al. 2022).
Clinical presentation
SS is a chronic inflammatory autoimmune disease. The clinical manifestations are variable:
“Although keratoconjunctivitis sicca and xerostomia are prominent symptoms, systemic symptoms such as skin lesions, Raynaud’s phenomenon, interstitial pneumonia, autonomic dysfunction and central nervous system dysfunction may also be present” (Ulusoy et al. 2022).
In 2002 the American-European Consensus Group published revised criteria for diagnosis of primary and secondary Sjögren syndrome (Vitali et al. 2002). These criteria, and the rules for classification, are summarized in the Tables below.
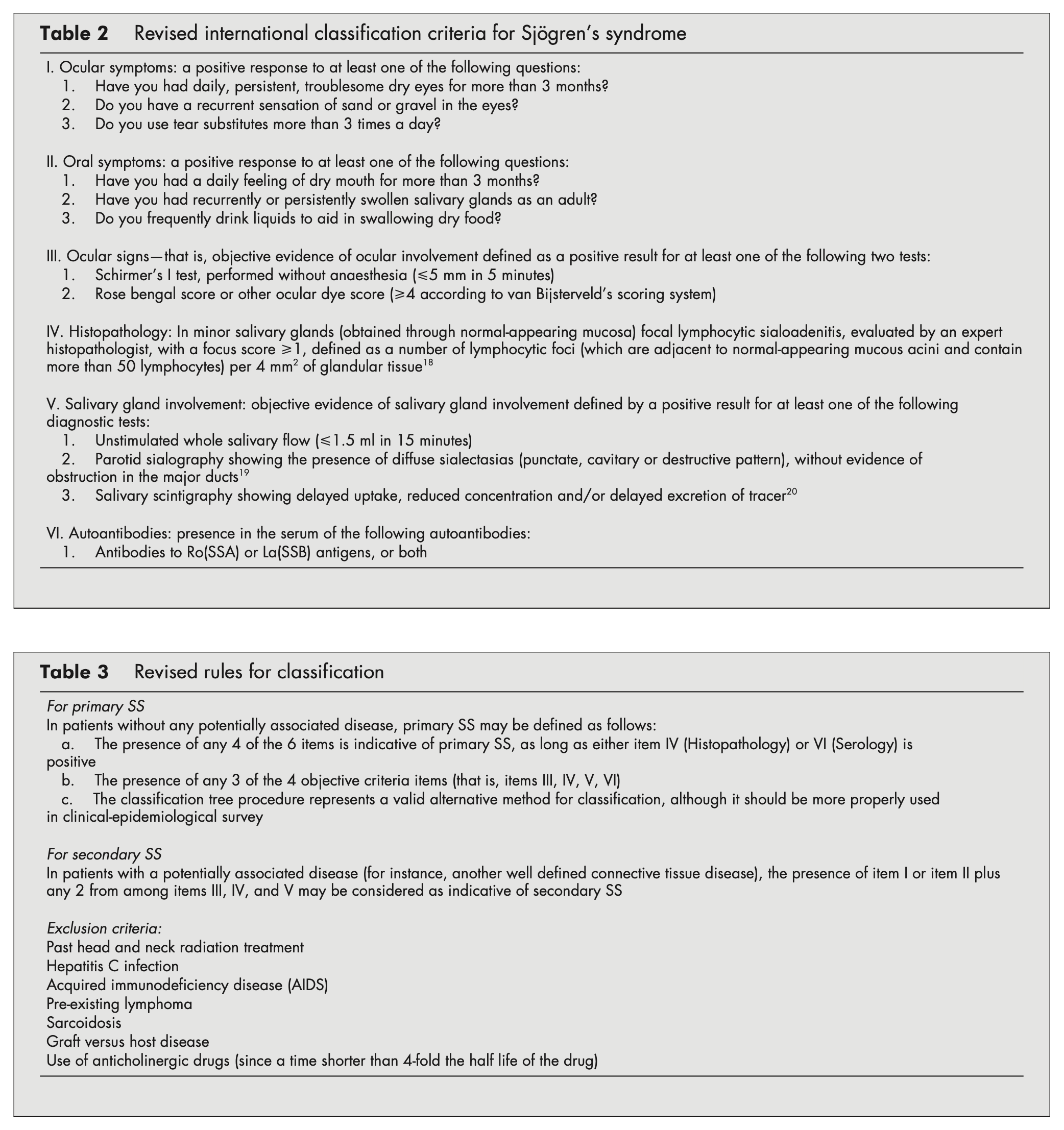
Other diagnostic criteria for SS include those published by the American College of Rheumatology and the European League Against Rheumatism (Shiboski et al. 2017a, b).
Involvement of the central nervous system in SS is somewhat uncommon. Ulusoy and colleagues state (Ulusoy et al. 2022):
“In primary Sjögren’s syndrome, the reported frequency of neurological symptoms varies between 8 and 49 per cent, with an average frequency of approximately 20 per cent. The most common peripheral neuropathies are distal sensor and sensorimotor neuropathies. Although cranial nerve mononeuropathy and polyneuropathy may be present, the most common neuropathy involving the craniofacial region is trigeminal neuropathy. Apart from the trigeminal nerve, involvement of VIIth, VIIIth, IIIrd, IVth and Vith cranial nerves have also been reported. Sensorineural hearing loss, especially at high frequencies, has been reported in patients. In addition to findings of vestibular involvement in primary Sjögren’s syndrome, some publications have reported vestibular preservation but with hearing dysfunction in primary Sjögren’s syndrome patients” (Ulusoy et al. 2022)
If a patient diagnosed with Sjögren syndrome complains of disequilibrium, potentially contributory factors (related to SS itself) include:
- Peripheral somatosensory neuropathy.
- Autonomic neuropathy causing orthostatic intolerance.
- Vestibular weakness (see below).
Physical examination
Physical examination findings vary depending on the organi system involved.
Ocular motor examination
In the case report by McCombe and colleagues (McCombe et al. 1992) of a 38-year-old man diagnosed with Sjögren syndrome who experienced an acute vestibular syndrome, the investigators stated that, “On examination, horizontal nystagmus was present for several weeks,” without further description.
Testing: auditory
Boki and colleagues (Boki et al. 2001) studied standard audiometry in 48 patients with primary Sjögren syndrome and compared them to 48 healthy control subjects. They reported that, “Significant differences in hearing loss were seen at 4000 Hz… and at 8000 Hz… Small differences in hearing acuity were also observed in the lower frequencies, but the absolute mean difference was <3 dB.”
Testing: caloric testing
Boki and colleagues (Boki et al. 2001) studied electronystagmography (ENG) in 10 patients with primary Sjögren syndrome (pSS) complaining of “dizziness and vertigo,” and compared them to 9 healthy controls. The investigators reported, “abnormalities for 4 of them: caloric responses were bilaterally reduced in 2 patients and unilaterally reduced in one patient, while positional nystagmus was documented in one patient.” They added that the, “Nine control subjects had similar complaints and 4 of them had an abnormal ENG evaluation,” though no further details were provided. In other words, there was a similar rate of “abnormalities” found in pSS patients versus controls.
McCombe and colleagues (McCombe et al. 1992) described the case of a 38-year-old man diagnosed with SS who developed severe somatosensory peripheral nerve involvement and autonomic dysfunction. Several months later he complained of “blurred vision and intermittent oscillopsia.” The investigators reported that, “Electronystagmography showed absent responses to caloric stimulation on two occasions” (McCombe et al. 1992).
Testing: vestibular evoked myogenic potentials (VEMP)
Ulusoy and colleagues (Ulusoy et al. 2022) studied vestibular evoked myogenic potentials (VEMP) in 30 women with primary Sjögren syndrome (pSS) and compared them to 35 healthy control subjects. They reported that:
- In cervical vestibular evoked myogenic potentials (cVEMP), the n1 latency was delayed compared to controls.
- In ocular vestibular evoked myogenic potentials (oVEMP), the p1n1 amplitude was larger compared to controls. They did not report thresholds.
The larger oVEMP amplitudes is difficult to explain. Enlarged VEMP amplitudes are generally found in third window phenomena, but no other evidence in support of this (such as low oVEMP thresholds) was described.
Testing: video head impulse testing (vHIT)
Ulusoy and colleagues (Ulusoy et al. 2022) studied video head impulse testing (vHIT) in 30 primary Sjögren syndrome (pSS) patients and compared them to 35 healthy control subjects. They reported low gain in the posterior and lateral semicircular canals compared to control subjects.
Testing: other
In patients complaining of dry eyes, an eye examination, undertaken by an ophthalmologist, should be able to quantify xerophthalmia with a Schirmer test.
In patients complaining of dry mouth, salivary gland function may be assessed by salivary gland biopsy or sialometry. Imaging by ultrasound or MRI may identify characteristic changes in the salivary gland parenchyma.
Serologic testing may identify anti-Ro/SSA and andi-La/SSB antibodies.
Imaging
Imaging of salivary glands (by ultrasound or MRI) is sometimes able to identify characteristic parenchymal changes.
Histopathology
Common histopathological findings in SS include “lymphocytic infiltration of the exocrine glands” (Ulusoy et al. 2022).
Differential diagnosis
The differential diagnosis of Sjögren syndrome is broad and includes other autoimmune diseases (Behcet disease, IgG4-related disease, sarcoidosis, systemic vasculitis) and autoimmune disorders (graft-versus-host disease), infectious causes (hepatitis C, HIV), lymphoma, medications and others.
Treatment
Management of a patient with SS is overseen by a rheumatologist, and requires a multidisciplinary approach when multiple organ systems are involved.
It would be extraordinarily unusual for an undiagnosed SS patient to present initially to a vestibular clinic. The more common scenario would be one in which a patient already diagnosed with SS complains of audiologic or vestibular symptoms or both, and the clinical query for an otoneurologist or neuro-otologist is whether those symptoms are from SS itself or due to some other independently occurring pathology. In such cases it is reasonable to seek more common causes of such symptoms (such as evaluating for benign paroxysmal positional vertigo). If workup identifies hearing loss, then referral to audiology is appropriate. If workup identifies vestibular weakness then it is medically reasonable to refer to vestibular rehabilitation therapy (VRT).
Prognosis
The prognosis of SS is quite variable, depending on many factors, including the specific organ systems affected.
References
Baldini C, Bombardieri S (2016) Chapter 1 – Introduction: History of Sjögren’s Syndrome. In: Gerli R, Bartoloni E, Alunno A (eds) Sjögren’s Syndrome. Academic Press, pp 1-9
Boki KA, Ioannidis JP, Segas JV, Maragkoudakis PV, Petrou D, Adamopoulos GK, Moutsopoulos HM (2001) How significant is sensorineural hearing loss in primary Sjogren’s syndrome? An individually matched case-control study. J Rheumatol 28: 798-801.
Ghafoor M (2012) Sjogren’s Before Sjogren: Did Henrik Sjogren (1899-1986) Really Discover Sjogren’s Disease? J Maxillofac Oral Surg 11: 373-4. doi: 10.1007/s12663-011-0303-0
Gougerot H (1890) Insuffisence progressive et atrophie des glandes salivaires ER muqueuses de la bouche, des conjonctives (et parfois des muqueuses nasale, laryngée, vulvaire). ‘Sécheresse’ de la bouche, des conjonctives, etc. [Progressive insufficiency and atrophy of the salivary glands ER mucous membranes of the mouth, conjunctivae (and sometimes nasal, laryngeal, vulvar mucous membranes). ‘Dryness’ of the mouth, conjunctivae, etc.]. Bulletin de la Société française de dermatologie et de syphiligraphie 32: 376-379.
Hadden W (1888) On ‘dry mouth’ or suppression of the salivary and buccal secretions. Trans Clin Soc Lond 21.
Jonsson R (2021) Henrik Sjogren (1899-1986): the syndrome and his legacy. Ann Rheum Dis 80: 1108-1109. doi: 10.1136/annrheumdis-2021-219942
Mavragani CP, Moutsopoulos HM (2010) The geoepidemiology of Sjogren’s syndrome. Autoimmun Rev 9: A305-10. doi: 10.1016/j.autrev.2009.11.004
McCombe PA, Sheean GL, McLaughlin DB, Pender MP (1992) Vestibular and ventilatory dysfunction in sensory and autonomic neuropathy associated with primary Sjorgren’s syndrome. J Neurol Neurosurg Psychiatry 55: 1211-2. doi: 10.1136/jnnp.55.12.1211
Mikulicz-Radecki JF (1888) [Concerning a peculiar symmetrical disease of the lacrimal and salivary glands]. Berlin Klin. Wschr: 759.
Mikulicz-Radecki JF (1892) Über eine eigenartige symmetrische Erkrankung der Thränen- und Mundspeicheldrüsen [Concerning a peculiar symmetrical disease of the lacrimal and salivary glands]. Beitr. z. Chir. Festschr. f. Theodor Billroth: 610-630.
Mulock-Houwer A (1927) Keratitis filamentosa and chronic arthritis. Trans Ophthal Soc UK 47: 88.
Shiboski CH, Shiboski SC, Seror R, Criswell LA, Labetoulle M, Lietman TM, Rasmussen A, Scofield H, Vitali C, Bowman SJ, Mariette X, International Sjogren’s Syndrome Criteria Working G (2017a) 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjogren’s Syndrome: A Consensus and Data-Driven Methodology Involving Three International Patient Cohorts. Arthritis Rheumatol 69: 35-45. doi: 10.1002/art.39859
Shiboski CH, Shiboski SC, Seror R, Criswell LA, Labetoulle M, Lietman TM, Rasmussen A, Scofield H, Vitali C, Bowman SJ, Mariette X, International Sjogren’s Syndrome Criteria Working G (2017b) 2016 American College of Rheumatology/European League Against Rheumatism classification criteria for primary Sjogren’s syndrome: A consensus and data-driven methodology involving three international patient cohorts. Ann Rheum Dis 76: 9-16. doi: 10.1136/annrheumdis-2016-210571
Sjögren HSC (1930) Keratoconjunctivitis sicca. Hygiea 92.
Sjögren HSC (1933) Zur Kenntnis der Keratoconjunctivitis sicca [Regarding keratoconjunctivitis sicca]. Acta Ophthalmol 11: 1-151.
Thorlacius GE, Bjork A, Wahren-Herlenius M (2023) Genetics and epigenetics of primary Sjogren syndrome: implications for future therapies. Nat Rev Rheumatol 19: 288-306. doi: 10.1038/s41584-023-00932-6
Ulusoy B, Limon M, Yilmaz S, Colpan B, Aygun AA, Korez MK, Erdur O (2022) Effects of primary Sjogren’s syndrome on hearing and vestibular systems. J Laryngol Otol 136: 1254-1258. doi: 10.1017/S0022215122000391
Vitali C, Bombardieri S, Jonsson R, Moutsopoulos HM, Alexander EL, Carsons SE, Daniels TE, Fox PC, Fox RI, Kassan SS, Pillemer SR, Talal N, Weisman MH, European Study Group on Classification Criteria for Sjogren’s S (2002) Classification criteria for Sjogren’s syndrome: a revised version of the European criteria proposed by the American-European Consensus Group. Ann Rheum Dis 61: 554-8. doi: 10.1136/ard.61.6.554
![]()