By Marcello Cherchi, MD PhD
For patients
Concussion can damage multiple parts of the head and brain, and thus can cause a variety of symptoms. Otoneurologists and neuro-otologists are usually tasked with assessing symptoms of hearing and balance. After physical examination, your physician may consider ordering audiologic and vestibular tests, and possibly imaging studies. Treatment and prognosis will depend on what specific deficits are discovered during the workup. Concussion can certainly cause deficits beyond hearing and balance, so it is important that a patient who has suffered concussion be evaluated at a center specializing in this area, because overall evaluation and management may require involvement of other specialties as well.
For clinicians
Overview
Concussion can cause a range of lesions. Lesions relevant to the audiovestibular system include otologic, neuro-ophthalmological, neurovascular, neurologic and others. Depending on the specific lesion(s), the clinical presentation and clinical examination will vary. Depending on the symptoms and physical examination findings, appropriate testing may include audiometry, vestibular evoked myogenic potentials, video head impulse testing, videonystagmography and rotatory chair testing. Imaging with MRI (brain and internal auditory canals) and temporal bone CT may be reasonable. Identification of specific deficits will guide treatment. Prognosis is as variable as the lesions themselves. What we have presented above pertains to the audiologic and vestibular consequences of concussion of interest to the otoneurologist; but concussion is a complex and incompletely understood phenomenon, and generally requires a multidisciplinary approach to diagnosis and management. In practice this usually requires referral to a center specializing in concussion/traumatic brain injury, which can coordinate the various evaluations and services needed to care for these patients.
Introduction
Concussion, generally classified as a sub-type of traumatic brain injury, is an immense topic. Head trauma is unfortunately common, and thus comprises a significant public health concern. Although concussion has attracted significant research interest, it remains incompletely understood; it lacks biomarkers for verification; convincing studies of effective treatments are lacking; and outcomes are sometimes poor.
Concussion can have a broad range of effects on the central nervous system, and we do not intend to present a comprehensive review here. Rather, we shall outline the otoneurologist’s role within what is usually a multidisciplinary approach to this problem.
Mechanisms of disequilibrium in the context of concussion
Head trauma can cause a variety of neurological lesions in the head and neck. Disequilibrium is fairly common in concussion, and it is on this symptom that we will focus, though this is not to suggest that other symptoms (headache, cognitive deficits) are unimportant.
- Otologic
- Benign paroxysmal positional vertigo
- Superior semicircular canal dehiscence
- Labyrinthine concussion, traction injury of the vestibulocochlear nerve
- Post-traumatic hydrops
- Neuro-ophthalmologic, particularly ocular motor disorders
- Trochlear nerve palsy or lateral rectus palsy
- Convergence insufficiency
- Accommodative insufficiency
- Saccadic deficits
- Neurovascular, e.g., vertebral artery dissection with embolization of the labyrinth
- Neurologic
- Post-traumatic migraine with migraine associated vertigo
- Cervicogenic vertigo
- Brainstem lesions
- Vestibular cortical lesions from shearing forces (at least in theory)
- Longer-term sequelae
- Persistent postural perceptual dizziness
- Visual vertigo
Otologic mechanisms
The most common cause of disequilibrium over the lifespan is benign paroxysmal positional vertigo (BPPV). The literature is mixed with respect to whether head trauma is a risk for BPPV. Several large studies conclude that head trauma is not a risk factor for BPPV (Aron, Lea et al. 2015, Luryi, LaRouere et al. 2019). Other studies conclude that head trauma is a risk factor for BPPV (Pisani, Mazzone et al. 2015), or that it increases the risk of specific variants of BPPV, such as anterior canal (Jackson, Morgan et al. 2007, Dlugaiczyk, Siebert et al. 2011) or bilateral involvement (Katsarkas 1999). Some studies conclude that head trauma appears to be associated with a higher risk of treatment failure in BPPV (Babac, Djeric et al. 2014, Balatsouras, Koukoutsis et al. 2017).
Head trauma can transmit sufficient kinetic energy to the labyrinth as to cause a labyrinthine concussion or traction injury of the vestibulocochlear nerve (Chiaramonte, Bonfiglio et al. 2013, Ishai, Knoll et al. 2018, Bartholomew, Lubner et al. 2020).
Head trauma can cause semicircular canal dehiscence, typically of the superior canal (McCrary, Babajanian et al. 2021).
Head trauma appears in some cases to result in endolymphatic hydrops (DiBiase and Arriaga 1997). This is sometimes referred to as “post-traumatic Ménière’s” (Gundrum 1959, Paparella and Mancini 1983, Lehrer and Poole 1984), but we prefer to reserve the term “Ménière’s” for the idiopathic syndrome. The mechanism of post-traumatic endolymphatic hydrops is unknown. Logically one would think that trauma causes disordered endolymphatic fluid flow, either from increased production, or decreased resorption, or both; this could in turn be due to alteration in the function of cells that produce these fluids, or in the hydraulic system through which they pass (cochlear duct, endolymphatic duct, and vestibular aqueduct).
Neuro-ophthalmologic mechanisms
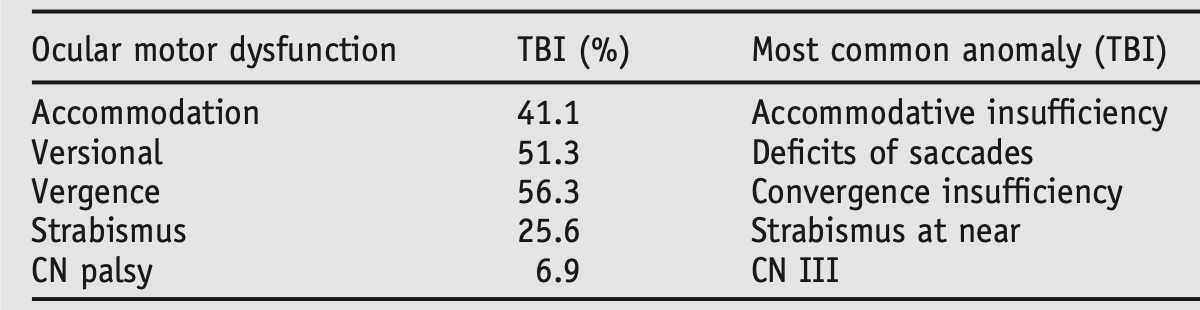
Ocular motor dysfunction is common after head trauma. This can result from extraocular muscle palsies, or from vergence deficits.
The Table below, from Ciuffreda and colleagues (Ciuffreda, Kapoor et al. 2007), shows the relative frequency of ocular motor abnormalities in a series of 160 patients who had suffered traumatic brain injury.
Neuro-vascular mechanisms
Head trauma can result in cervical arterial dissections. Dissection of the vertebral artery, in particular, can predispose to embolization of the labyrinthine artery (usually via the anterior inferior cerebellar artery), resulting in labyrinthine ischemia/infarction (Choi, Chun et al. 2006, Eliezer, Verillaud et al. 2019). Embolization to any of the cerebellar arteries can also result in cerebellar infarction (Kim, Kosnik et al. 1997, Tabuchi and Nakayasu 2015, Ilker Oz, Bozay Oz et al. 2016).
Neurologic mechanisms
Migraines can develop (or recur) following concussion, and this can include migraine associated vertigo.
Concussion is often associated with neck trauma, which in turn can predispose to cervicogenic vertigo (Cherchi, DiLiberto et al. 2021).
The actual “brain damage” in concussion probably has multiple mechanisms, such as shearing forces exerted on gray and white matter, resulting in a variety of cellular dysfunctions. Magnetic resonance tractography is an evolving imaging modality for this disease process. In patients with post-concussive disequilibrium, research has identified damage to tracts relevant to vestibular function (Jang, Bae et al. 2021).
Vestibular cortex in the temporal lobe (Vidal, De Waele et al. 1999, de Waele, Baudonniere et al. 2001) can be damaged in concussion. At least in theory, such lesions could give rise to disequilibrium. This has not been addressed in published studies.
Longer-term sequelae
Nearly any cause of disequilibrium can secondarily give rise to persistent postural perceptual dizziness (PPPD).
Similarly, visual vertigo (VV) can superimpose itself on other, pre-existing sources of disequilibrium, including post-concussive disequilibrium.
Presentation
The presentation of post-concussive disequilibrium depends on the consequent lesions.
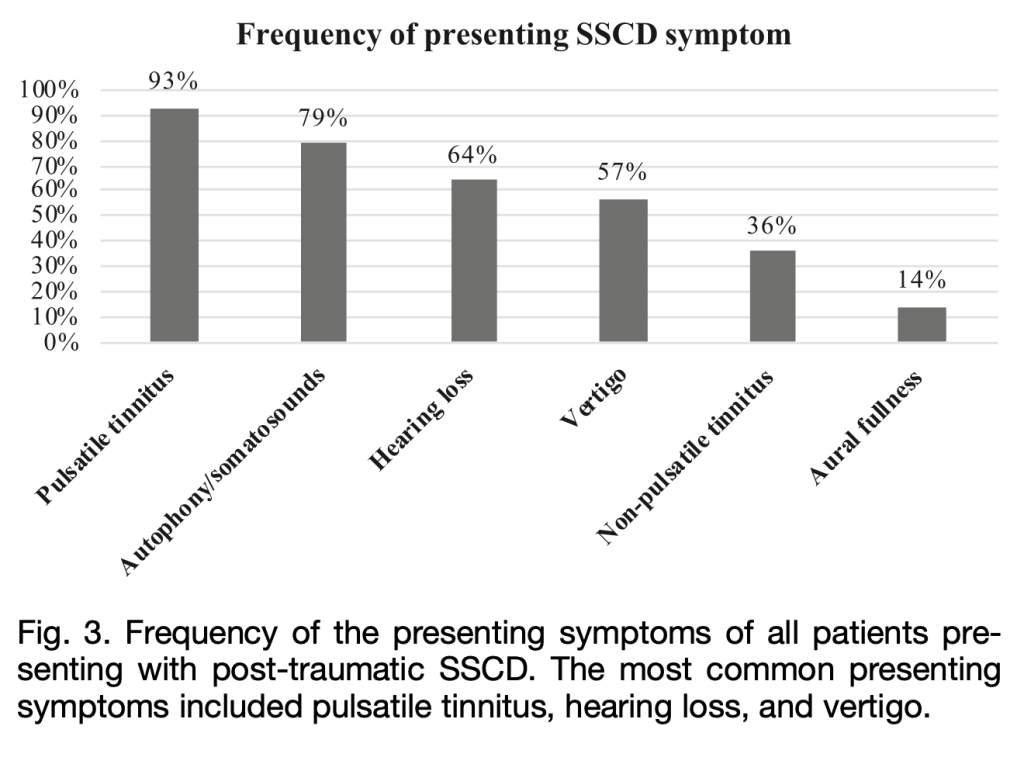
The Figure below shows the relative frequency of symptoms in post-traumatic superior semicircular canal dehiscence in the series studied by McCrary and colleagues (McCrary, Babajanian et al. 2021).
Physical examination
In patients who have suffered head trauma, some physical examination findings may be suggestive of temporal bone fracture, such as ecchymosis over the mastoid process — sometimes called Battle’s sign (Battle 1890) — periorbital ecchymosis, or hemotympanum.
In patients who have suffered concussion and present with auditory and/or vestibular symptoms, physical examination findings will depend on the particular lesions.
Of otologic mechanisms, benign paroxysmal positional vertigo may be detectable on ocular motor examination. Unilateral vestibular weakness (such as from traction injury of the vestibulocochlear nerve, or labyrinthine infarction) may manifest with spontaneous horizontal nystagmus. Hearing loss may be evident on examination.
Of neuro-ophthalmologic mechanisms, ocular motor dysfunction may be evident on physical examination, ranging from saccadic deficiencies, vergence abnormalities or strabismus.
Testing
Audiologic testing may show sensorineural hearing loss compatible with labyrinthine concussion, or conductive hyperacusis compatible with superior semicircular canal dehiscence.
Cervical and/or ocular vestibular evoked myogenic potentials may show findings compatible with superior semicircular canal dehiscence (Fife, Colebatch et al. 2017).
Unilateral vestibular weakness may be detected on vestibular evoked myogenic potentials, video head impulse testing or caloric testing.
Bilateral vestibular weakness may be detected on rotatory chair testing.
More detailed ocular motor studies are being researched for concussion, but remain investigational. For example, the Figure below, from Wetzel and colleagues (Wetzel, Lindblad et al. 2018), compares sinusoidal smooth pursuit in a control subject (upper panel) versus a patient who suffered concussion (lower panel).
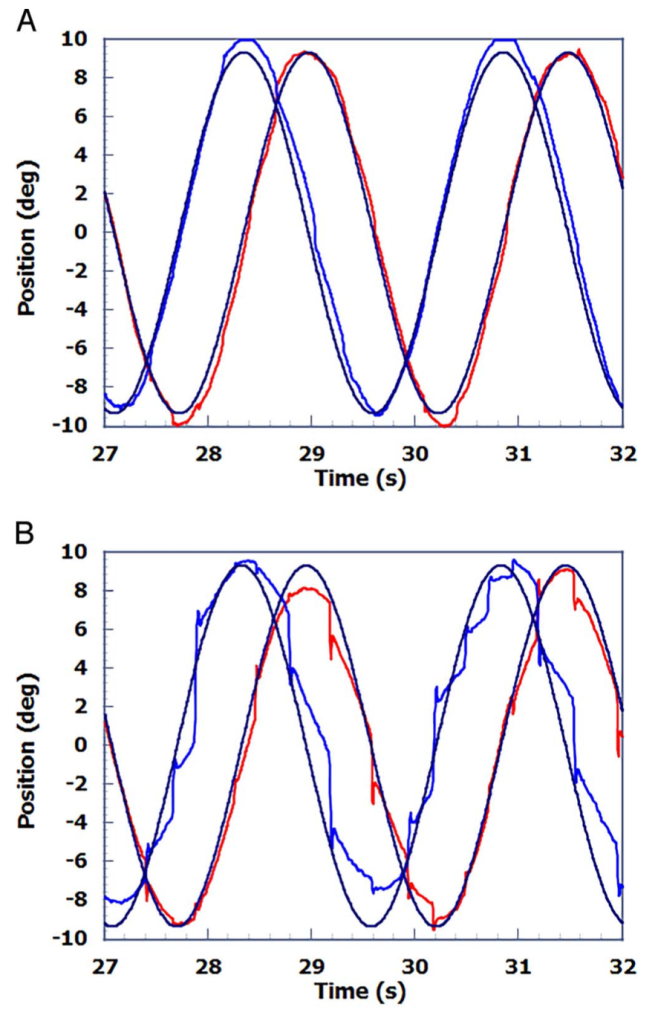
Figure : Sinusoidal smooth pursuit in a control subject (upper panel) compared to a patient who suffered concussion (lower panel). From Wetzel et al. 2018.
Imaging
Brain imaging in a patient with concussion may in some instances identify a discrete lesion that could account for auditory and/or vestibular symptoms. For example, MRI of the brain and internal auditory canals may identify labyrinthine hemorrhage or cerebellar infarction. Temporal bone CT may identify a temporal bone fracture or superior semicircular canal dehiscence.
But brain imaging in a patient with concussion is also necessary to evaluate for other findings that may reflect more severe traumatic brain injury, such as a parenchymal hematoma or subarachnoid hemorrhage.
Treatment
Treatment of post-concussive disequilibrium depends on the specific lesion, if identifiable.
If an identified vestibular deficit is one that is usually treated with vestibular rehabilitation, then the same principles can apply in the context of post-concussion disequilibrium (Gurley, Hujsak et al. 2013).
Benign paroxysmal positional vertigo occurring in the context of concussion is treated the same as idiopathic BPPV (Ouchterlony, Masanic et al. 2016). Some studies conclude that head trauma appears to be associated with a higher risk of treatment failure in BPPV (Babac, Djeric et al. 2014, Balatsouras, Koukoutsis et al. 2017).
Hearing loss, such as from labyrinthine concussion, may be aidable with amplification.
Prognosis
Post-concussive disequilibrium “may resolve in days to weeks, or persist for months to years” (Hac and Gold 2022). This variability is partly due to the range of mechanisms discussed above.
References
Aron M, Lea J, Nakku D, Westerberg BD (2015) Symptom Resolution Rates of Posttraumatic versus Nontraumatic Benign Paroxysmal Positional Vertigo: A Systematic Review. Otolaryngol Head Neck Surg 153: 721-30. doi: 10.1177/0194599815594384
Babac S, Djeric D, Petrovic-Lazic M, Arsovic N, Mikic A (2014) Why do treatment failure and recurrences of benign paroxysmal positional vertigo occur? Otol Neurotol 35: 1105-10. doi: 10.1097/MAO.0000000000000417
Balatsouras DG, Koukoutsis G, Aspris A, Fassolis A, Moukos A, Economou NC, Katotomichelakis M (2017) Benign Paroxysmal Positional Vertigo Secondary to Mild Head Trauma. Ann Otol Rhinol Laryngol 126: 54-60. doi: 10.1177/0003489416674961
Bartholomew RA, Lubner RJ, Knoll RM, Ghanad I, Jung D, Nadol JB, Jr., Alvarez VE, Remenschneider A, Kozin ED (2020) Labyrinthine concussion: Historic otopathologic antecedents of a challenging diagnosis. Laryngoscope Investig Otolaryngol 5: 267-277. doi: 10.1002/lio2.360
Battle WH (1890) Three Lectures on Some Points Relating to Injuries to the Head. Br Med J 2: 141-7. doi: 10.1136/bmj.2.1542.141
Cherchi M, DiLiberto FE, Yacovino DA, Das S (2021) The Enduring Controversy of Cervicogenic Vertigo, and Its Place among Positional Vertigo Syndromes. Audiology Research 11: 491-507. doi: 10.3390/audiolres11040045
Chiaramonte R, Bonfiglio M, D’Amore A, Viglianesi A, Cavallaro T, Chiaramonte I (2013) Traumatic labyrinthine concussion in a patient with sensorineural hearing loss. Neuroradiol J 26: 52-5. doi: 10.1177/197140091302600109
Choi KD, Chun JU, Han MG, Park SH, Kim JS (2006) Embolic internal auditory artery infarction from vertebral artery dissection. J Neurol Sci 246: 169-72. doi: 10.1016/j.jns.2006.02.014
Ciuffreda KJ, Kapoor N, Rutner D, Suchoff IB, Han ME, Craig S (2007) Occurrence of oculomotor dysfunctions in acquired brain injury: a retrospective analysis. Optometry 78: 155-61. doi: 10.1016/j.optm.2006.11.011
de Waele C, Baudonniere PM, Lepecq JC, Tran Ba Huy P, Vidal PP (2001) Vestibular projections in the human cortex. Exp Brain Res 141: 541-51. doi: 10.1007/s00221-001-0894-7
DiBiase P, Arriaga MA (1997) Post-traumatic hydrops. Otolaryngol Clin North Am 30: 1117-22.
Dlugaiczyk J, Siebert S, Hecker DJ, Brase C, Schick B (2011) Involvement of the anterior semicircular canal in posttraumatic benign paroxysmal positioning vertigo. Otol Neurotol 32: 1285-90. doi: 10.1097/MAO.0b013e31822e94d9
Eliezer M, Verillaud B, Guichard JP, Kania R, Toupet M, Herman P, Houdart E, Hautefort C (2019) Labyrinthine infarction caused by vertebral artery dissection: consideration based on MRI. J Neurol 266: 2575-2577. doi: 10.1007/s00415-019-09456-0
Fife TD, Colebatch JG, Kerber KA, Brantberg K, Strupp M, Lee H, Walker MF, Ashman E, Fletcher J, Callaghan B, Gloss DS, 2nd (2017) Practice guideline: Cervical and ocular vestibular evoked myogenic potential testing: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 89: 2288-2296. doi: 10.1212/WNL.0000000000004690
Gundrum LK (1959) Post-traumatic Meniere’s symptom-complex. Eye Ear Nose Throat Mon 38: 385-8.
Gurley JM, Hujsak BD, Kelly JL (2013) Vestibular rehabilitation following mild traumatic brain injury. NeuroRehabilitation 32: 519-28. doi: 10.3233/NRE-130874
Hac NEF, Gold DR (2022) Neuro-Visual and Vestibular Manifestations of Concussion and Mild TBI. Curr Neurol Neurosci Rep. doi: 10.1007/s11910-022-01184-9
Ilker Oz I, Bozay Oz E, Serifoglu I, Kaya N, Erdem O (2016) Cerebellar Infarction in Childhood: Delayed-Onset Complication of Mild Head Trauma. Iran J Child Neurol 10: 82-5.
Ishai R, Knoll RM, Chen JX, Wong K, Reinshagen KL, Nadol JB, Jr., Remenschneider AK, Jung DH, Kozin ED (2018) Otopathologic Changes in the Cochlea following Head Injury without Temporal Bone Fracture. Otolaryngol Head Neck Surg 159: 526-534. doi: 10.1177/0194599818769861
Jackson LE, Morgan B, Fletcher JC, Jr., Krueger WW (2007) Anterior canal benign paroxysmal positional vertigo: an underappreciated entity. Otol Neurotol 28: 218-22. doi: 10.1097/01.mao.0000247825.90774.6b
Jang SH, Bae CH, Kim JW, Kwon HG (2021) Relationship between Dizziness and the Core Vestibular Projection Injury in Patients with Mild Traumatic Brain Injury. Diagnostics (Basel) 11. doi: 10.3390/diagnostics11112070
Katsarkas A (1999) Benign paroxysmal positional vertigo (BPPV): idiopathic versus post-traumatic. Acta Otolaryngol 119: 745-9. doi: 10.1080/00016489950180360
Kim SH, Kosnik E, Madden C, Rusin J, Wack D, Bartkowski H (1997) Cerebellar infarction from a traumatic vertebral artery dissection in a child. Pediatr Neurosurg 27: 71-7. doi: 10.1159/000121230
Lehrer JF, Poole DC (1984) Post-traumatic Meniere’s syndrome. Laryngoscope 94: 129. doi: 10.1288/00005537-198401000-00025
Luryi AL, LaRouere M, Babu S, Bojrab DI, Zappia J, Sargent EW, Schutt CA (2019) Traumatic versus Idiopathic Benign Positional Vertigo: Analysis of Disease, Treatment, and Outcome Characteristics. Otolaryngol Head Neck Surg 160: 131-136. doi: 10.1177/0194599818797892
McCrary HC, Babajanian E, Patel N, Yang S, Kircher M, Carlson ML, Gurgel RK (2021) Superior Semicircular Canal Dehiscence Syndrome Following Head Trauma: A Multi-institutional Review. Laryngoscope 131: E2810-E2818. doi: 10.1002/lary.29751
Ouchterlony D, Masanic C, Michalak A, Topolovec-Vranic J, Rutka JA (2016) Treating Benign Paroxysmal Positional Vertigo in the Patient With Traumatic Brain Injury: Effectiveness of the Canalith Repositioning Procedure. J Neurosci Nurs 48: 90-9; quiz E1. doi: 10.1097/JNN.0000000000000186
Paparella MM, Mancini F (1983) Trauma and Meniere’s syndrome. Laryngoscope 93: 1004-12. doi: 10.1288/00005537-198308000-00006
Pisani V, Mazzone S, Di Mauro R, Giacomini PG, Di Girolamo S (2015) A survey of the nature of trauma of post-traumatic benign paroxysmal positional vertigo. Int J Audiol 54: 329-33. doi: 10.3109/14992027.2014.989454
Tabuchi S, Nakayasu H (2015) Traumatic vertebral artery dissection and cerebral infarction following head and neck injury with a lucid interval. Acute Med Surg 2: 127-130. doi: 10.1002/ams2.75
Vidal PP, De Waele C, Baudonniere PM, Lepecq JC, Ba Huy PT (1999) Vestibular projections in the human cortex. Ann N Y Acad Sci 871: 455-7.
Wetzel PA, Lindblad AS, Raizada H, James N, Mulatya C, Kannan MA, Villamar Z, Gitchel GT, Weaver LK (2018) Eye Tracking Results in Postconcussive Syndrome Versus Normative Participants. Invest Ophthalmol Vis Sci 59: 4011-4019. doi: 10.1167/iovs.18-23815
![]()